In This Issue
Message From the
Executive Director
 Now Visit VSI Now Visit VSI
on Facebook
 And Twitter And Twitter
Support VSI Today
Advocacy: Legislation
You Need to Know About
- Insurance Network Narrowing
Could Remove YOUR Doctor
- Are Dermatologists Being Targeted?
Save the Date!
2015 Conference
Repigmentation Patterns:
What to Expect
What's On Your Mind?
- Is Green Tea Good
for Vitiligo?
Medical News Updates
- A Test for Vitiligo
Susceptibility?
- Green Tea and Vitiligo
- Metabolic Syndrome
- Autoimmune Thyroid
and White Hair
- ReCell Update
- Clinuvel-Scenesse
Phase I Trial Results
Research & Clinical Trials
Bibliography
New! Support VSI With eBay
Earn funding for VSI
When you Shop!
View Past Newsletters
- Summer Edition 2014
- Spring Edition 2014
- Winter Edition 2013
- Fall Edition 2013
- Summer Edition 2013
- Spring Edition 2013
- Winter Edition 2012
- Fall Edition 2012
- Summer Edition 2012
- Spring Edition 2012
- Winter Edition 2011
- Fall Edition 2011
- Spring Edition 2011
VSI Medical and Scientific
Advisory Committee
Pearl E. Grimes, M.D., Committee Chair
Ted A. Grossbart, Ph.D.
Sancy A. Leachman, M.D.
I. Caroline Le Poole Ph.D.
Mauro Picardo, M.D.
Nanette B. Silverberg, M.D.
Richard A. Spritz, M.D.
Alain Taieb, M.D., Ph.D.
Wiete Westerhof, MD, Ph.D.
For more information
on VSI's MSAC Click Here |
| |
| |
How to Log In:
Have you have forgotten your Login ID and/or Password?
No Problem!
Just go to the
Community Page
Scroll down to
the login box.
LOOK UNDERNEATH!
You'll see instructions to have them sent to the email address on your account. |
|
How to Log In:
Have you have forgotten your Login ID and/or Password?
No Problem!
Just go to the
Community Page
Scroll down to
the login box.
LOOK UNDERNEATH!
You'll see instructions to have them sent to the email address on your account.
|
|
How to Log In:
Have you have forgotten your Login ID and/or Password?
No Problem!
Just go to the
Community Page
Scroll down to
the login box.
LOOK UNDERNEATH!
You'll see instructions to have them sent to the email address on your account.
|
|
How to Log In:
Have you have forgotten your Login ID and/or Password?
No Problem!
Just go to the
Community Page
Scroll down to
the login box.
LOOK UNDERNEATH!
You'll see instructions to have them sent to the email address on your account.
|
|
How to Log In:
Have you have forgotten your Login ID and/or Password?
No Problem!
Just go to the
Community Page
Scroll down to
the login box.
LOOK UNDERNEATH!
You'll see instructions to have them sent to the email address on your account.
|
|
| |
| Contact Us
Online
VitiligoSupport.org
Email Contact Us
Postal Mail Address
Vitiligo Support International
P.O. Box 3565
Lynchburg Va 24503
Phone
(434) 326-5380 |
|
|
Message From the Executive Director

 Dear Members and Friends of VSI, Dear Members and Friends of VSI,
In addition to being your advocate in the clinical, research and government arenas, one of the most important things VSI can do for vitiligo patients is to actively remain on top of the latest information, share it with you, and find the answers to the your questions – all to encourage you to take charge of your life, and join with VSI in the fight for better knowledge and treatment! We not only want to make sure you are armed with the latest knowledge to treat, manage and understand your disease, but we want to let you know what VSI is doing to improve your future and how you can become involved to ensure this happens.
We regularly receive questions about repigmentation, so we decided to “go back to school” this fall, providing a primer on the different types of repigmentation and what you can expect from repigmentation therapies. In our "Medical News Updates" column, we move beyond the skin manifestations to look at potential complications throughout the body, including new studies on metabolic abnormalities that can occur in vitiligo, such as abnormal cholesterol, glucose intolerance and increased homocysteine levels that can lead to cardiovascular risks.
Government advocacy is of great importance for making progress for any disease! In September, as part of a major initiative led by the American Academy of Dermatology, I joined dermatologists and related healthcare professionals on Capitol Hill to ensure that our national legislators are aware of the needs of vitiligo patients. One of the major topics was the need to ensure that insurance companies allow access to the specialized care required for vitiligo.
Without VSI advocating on behalf of vitiligo patients, I’m afraid to think of the laws that might be passed restricting our care and the research funding that is our hope for the future.
This brings us to a critical subject:
VSI cannot advocate, educate, and provide support without your financial help.
We do this for YOU!
Would you like to see more research for vitiligo?
Would you like to have better treatments for vitiligo?
Would you like to have vitiligo treatments routinely covered by insurance?
Would you like more dermatologists to be aware of the current treatments for vitiligo?
Would you like dermatologists, the insurance industry and the general public to have a better understanding of the impact this disease has on those affected?
Do you want to know about new research efforts?
Do you want to know about new vitiligo treatments in the pipeline?
Do you want to know about potential legislation that could impact or remove
your personal choices for acquiring the best and most appropriate treatment?
Effort on each of these fronts requires funding.
If vitiligo is to ever have the level of representation necessary to make a difference in your life and your future, then you must personally commit to financially support VSI, the only organization representing your interests on the forefront of this battlefield.
Running an organization costs money;
Running an organization WELL -- costs a lot more.
Sincerely,
Jackie Gardner
Executive Director
If You Are Not A Supporting Member Of VSI,
What Are You Waiting For?
Please - Give Us Something To Fight With.
The Time To Invest In Your Future Is Now.
Become a Supporting Member: Click Here
Make a General Donation Through VSI: Click Here
Make a General Donation with PayPal.
|

|
This organization is a Silver-level GuideStar Exchange
participant, demonstrating its commitment to transparency. |

Advocacy and Legislation:

VSI director Jackie Gardner recently attended the
American Academy of Dermatology Association's
Legislative Conference in Washington, DC from
Sept 7-9. She and 139 dermatologists, residents,
patients’ advocates, and dermatology nurses met with
189 members of Congress, from 31 states.
The Primary Messages This Year:
1. Patient Access to Care and Network Adequacy
2. Increased Medical Research Funding
How does this affect you?
One of the most often requested services of VSI is help locating a dermatologist knowledgeable of, and willing to prescribe current treatments. If you are reading this, you are very likely aware of this problem. Well, believe it or not, this situation is about to get worse.
Vitiligo patients already routinely face waiting periods up to, or over 6 months to find a dermatologist willing to prescribe a treatment for them, and now- without cause and without warning, the doctor they are seeing can be dropped MID-CYCLE from the insurance network.
Is it OK with you for your insurance company to decide if you can see a specialist?
Does your primary care physician know the difference between vitiligo and many of the other skin disorders causing depigmentation? Does he/she have a NB-UVB lightbox, or know about current vitiligo treatments? Probably not. Yet United Health, one of Medicare's largest insurance providers now admits that they are "encouraging the use of primary care." A June 2014 report noted dermatologists as among those being targeted for termination.
Medicare Advantage is now dropping doctors from networks without warning, and in some cases admittedly "without cause." In fact, many of the termination notices arrive in unmarked envelopes as bulk mail. Does that sound like an “above-board” procedure? This new trend known as "economic credentialing" is unabashedly removing doctors from networks without regard to the individual physician’s qualifications, quality of care, or professional competency, strictly as a "cost saving" measure. Doctors who are willing to offer expensive therapies, or prescribe expensive treatments, are being terminated from the network with no meaningful review or appeal process.
Will this affect me if I do not have Medicare or Medicare Advantage?
You may think that because you do not yet have to rely on Medicare for your insurance that this does not affect you. However, what you may not realize is that in the United States, 54 million Americans are now covered by Medicare or Medicare Advantage, making it the nation’s largest health insurance program. Consequently, many, if not most, insurance providers establish their baseline standards and procedures to follow the Medicare model.
We cannot stand by and let this happen.
Please read the following information carefully,
then make your voice heard on this matter.
The Time To Act Is Now.
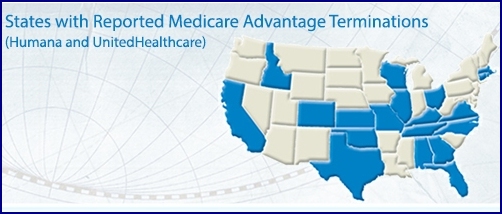
Patient Access To Care & Network Adequacy:

Medicare Advantage (MA) (Part C) is a health insurance alternative to traditional Medicare (Part A & B). Offered through private health plans, MA plans provide benefits through local Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs), and Private Fee-For-Service (PFFS) plans.
Thousands of physicians across the country have been terminated from MA networks from a variety of insurance carriers. Dermatologists in at least 17 states have been dropped without cause from at least two MA network plans. To the detriment of Medicare patients, these actions threaten patient access and fail to meet the network adequacy standards of the MA program.
Health plan networks should exist to serve patient needs, specifically by guaranteeing that patients have adequate and timely access to physicians with appropriate training and specialty or subspecialty expertise. To this end, health plans should be required to provide the following:
- Access to Care: Networks should ensure that physicians are available to patients. Plans should be required to demonstrate that their physician network is adequate by including relevant metrics by geographic region on provider availability and provider subspecialty.
- Accurate and Timely Information: Patients should have access to complete, updated lists of current medical specialties, subspecialties, and practice focuses.
- Transparency: Patients should be provided reasonable and adequate notice if their physician is being terminated from a plan prior to Open Enrollment periods.
- Fair Appeals Process: Physicians should be provided a fair, meaningful, and timely appeal whenever a physician is terminated from a network, regardless of how the plan characterizes the termination, and the process should consider whether the removal of the physician from the network would result in network inadequacy.
*Above information from the American Academy of Dermatology Association
What Can You Do?
You must be a legal resident of the United States in order to weigh in on these measures.

Using the links provided below, contact your members of the
House of Representatives, and Senate.
It is important to cite the appropriate “House” (H.R.) or “Senate” (S.) legislation.
1. Tell them how these measures could affect you and your health,
2. Then include the appropriate House, or Senate message below.
House of Representatives:
If you have not already done so, I respectfully urge you to cosponsor H.R. 4998: The Medicare Advantage Participant Bill of Rights Act,which makes certain that provider networks cannot be changed mid-year by terminating physicians without cause, andthat networks will be finalized before open enrollment begins.
Senate:
If you have not already done so, I respectfully urge you to cosponsor S. 2552: The Medicare Advantage Participant Bill of Rights Act, which makes certain that provider networkscannot be changed mid-year by terminating physicians without cause, andthat networks will be finalized before open enrollment begins.
Medical Research Funding:
At any given time, 1 in 3 Americans suffers from a skin disease. Some of these are chronic inflammatory, multi-system, disabling and life-threatening conditions. Under the current budget, the NIH funding was cut by $1.03 billion.
House of Representatives:
If you have not already done so, I respectfully urge you to prioritize federal investment in medical research and cosponsor HR 460, the Patients’ Access to Treatment Act, which will enable patients to access treatments, reduce disability and constrain health care costs.
Senate:
If you have not already done so, I respectfully urge you to prioritize federal investment in medical research; and learn more about cost barriers to certain medications and consider being the lead Senate sponsor of the Patients’ Access to Treatments Act.
*Above information from the American Academy of Dermatology Association
Contact Your Legislators!
Most legislators provide a form that you can fill in on their website.
It’s easiest if you compose your message first, so that you can
copy and paste it into the provided form.
To Locate Your:
Members of the House of Representatives: Click Here
Senators: Click Here
|
Back to Top
2015 Vitiligo Conference!
Mark Your Calendars Now – Save The Date!
2015 Vitiligo Conference
9/26/15 – 9/27/15
Orange California

Details will be announced in future newsletters,
on VSI's website, and via VSI's social media channels.
To Receive Announcements and
Advance Meeting Information:
Click Here
Repigmentation Patterns:
Repigmentation: How is Pigment Generated?
Mainstream treatments for vitiligo typically focus on regenerating lost pigment. Because cells that produce pigment are targeted in vitiligo, with many of those cells eventually being destroyed, therapies that are currently available to treat vitiligo have been geared toward activating the generation of new pigment (repigmentation). But how does this regeneration actually happen? Vitiligo patients frequently ask us questions such as: What will new pigment look like? How fast will the treatment work? How long will the new pigment last? This article attempts to answer those questions.
When first diagnosed with vitiligo, many people envision the repigmentation process as being similar to getting a suntan - expose the skin to ultraviolet light, and the depigmented areas will "tan" or automatically and completely fill in. But, unfortunately, it's not that simple. To help our readers understand how repigmentation actually happens, we'll take you through a brief introduction about the elements and processes that are necessary for repigmentation to take place. We'll then talk about what the new pigment will look like, how the pigment fills in and the different patterns that can result. Finally, we’ll report on how therapies activate repigmentation, how quickly that can occur and how stable the results might be.
Melanocytes:
To understand the different ways repigmentation can occur, it's important to understand the elements involved in the process of pigmentation. First, we must have melanocytes, which are the cells that produce melanin, or pigment, and exist to absorb ultraviolet light so that damaging rays don't penetrate past the skin. These cells are mostly found in hair follicles but can also be found in the outer layer of the skin, or epidermis. This latter fact is important because melanocytes that are located along the edges of vitiligo lesions and even those that can still be present within a depigmented area, including years after the area first becomes depigmented, can be activated to once again produce pigment.
While melanocytes are the primary source of pigmentation, other elements contribute to the generation of new pigment as well. For example, keratinocytes contribute to the stability of melanocytes and help stimulate and regulate the growth of melanocytes. Cytokines are proteins that are important in cell-to-cell communication. Finally, ultraviolet light and oral and topical therapies can activate the production of pigmentation.
Terms to Know
Hair Follicle -- a small cavity in the epidermis region of the skin, from which a
hair develops, and where the majority of pigment cells are produced
Melanin -- the color, or pigment, that is responsible for the color of
our skin, hair and eyes and darkens the skin to protect us from sun damage
Melanocyte -- a cell that produces melanin which is the pigment responsible
for skin color
Melanocyte Reservoir -- a place in the hair follicle where melanocytes
are produced
Pigmentation -- the coloring of the skin, hair, mucous membranes,
and the retina of the eye
Repigmentation -- the process of regenerating pigment after pigment
has been depleted
Hyperpigmentation -- too much pigment caused by increased melanin,
resulting in darker pigment on an area of the skin
Hypopigmentation -- too little pigment, causing skin lightening
Depigmentation – loss of pigment
Keratinocyte -- the predominant cell type in the outer layer of the skin, or epidermis
Cytokine – a protein that acts as a messenger between cells and facilitates
communication between immune cells (an important process, for example, in
pigmentation), but may also be responsible for increasing inflammation in
autoimmune disease |
The Importance of the Hair Follicle
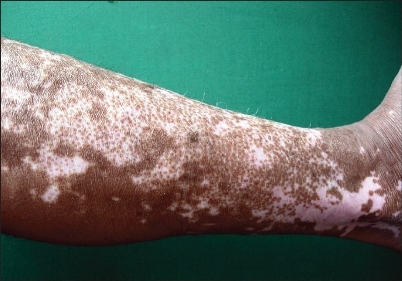
The vast majority of melanocytes are produced within the tiny hair follicles, then migrate to the outer layer of the skin. These melanocytes also provide hair with its color. Some depigmented areas have enough functioning melanocytes to retain the natural hair color coming from those hair follicles. However, in some instances, so many of the functional melanocytes have been destroyed that the hair also loses its color. Both pigmented and depigmented hair can be seen in the photo of the vitiligo patient below.

Copyright© Indian Journal of Dermatology; Reprinted with appreciation for the permission
provided by the open access 2009 article by R Fabella.
The importance of the hair follicle as a reservoir of melanocytes means that regenerating pigment on areas where hair follicles are absent, such as on the palms of the hands; soles of the feet; and mucosal areas, becomes much more difficult.
Patterns of Repigmentation
Now that we have talked about where melanocytes can be found, let’s explore the patterns of repigmentation and some of the factors involved. Pigment originating from hair follicles leads to a "perifollicular" or "follicular" pattern and appears as a small dot or freckle emerging from the hair follicle inside the depigmented area. “Marginal” repigmentation, also referred to as "border spreading," actually begins on the outer edges, or border of the lesion and fills from the outside, so that the lesion slowly becomes smaller and smaller. The third pattern, known as “diffuse” repigmentation, is when new pigment does not come from the hair follicle, but is recruited from nearby melanocytes in the skin of the lesion. Though this type of repigmentation appears on the inside of the lesion, because it does not originate in the hair follicle, the appearance will be more like small islands of color, rather than a dot or freckle coming from the hair follicle. In each of these cases, whether from one process or a combination of patterns and processes, the pigment grows and spreads, eventually merging together to repigment the lesion.
The Following Photographs Show Repigmentation Patterns
Figure 1 - Perifollicular Repigmentation
Copyright© Indian Journal of Dermatology; Reprinted with appreciation for the permission
provided by the open access 2009 article by R Fabella.
Figure 2 - Marginal Repigmentation

Copyright© Indian Journal of Dermatology; Reprinted with appreciation for the permission
provided by the open access 2009 article by R Fabella.
Figure 3 - Diffuse Repigmentation

Copyright© Indian Journal of Dermatology; Reprinted with appreciation for the permission
provided by the open access 2009 article by R Fabella.
Speed and Stability
Of great interest to vitiligo patients is the speed with which a specific therapy can regenerate pigment and how stable the pigment is once it is newly generated. These are questions that clearly need further study, but at least these important issues were brought to the fore in a 2004 publication by researchers in India.
Dr. Parsad and colleagues followed 125 vitiligo patients who used topical or systemic psoralens (PUVA) and/or topical or oral steroids and/or topical calcipotriol, or only topical steroids. PUVA, at least in the United States, has now largely been replaced by narrow-band ultraviolet B light (NB-UVB) photo therapy, which has been deemed more effective and less damaging to the skin, with fewer side effects. Calcipotriol and other variations of vitamin D derivatives are frequently used in combination with other topicals, including Taclonex, and light therapy.
Patients were checked at 3 months to determine how quickly repigmentation occurred and again at 6 months, after therapy had ceased, to assess retention of the new pigment. As expected, perifollicular repigmentation occurred most frequently, followed by diffuse and then marginal. Most interesting was the speed and stability of the repigmentation for each pattern. Pigment appeared fastest in the diffuse pattern, but it was the least stable of all of the repigmentation patterns. The marginal pattern was the most stable but the slowest to evolve. The perifollicular pattern came in second for both speed and stability.
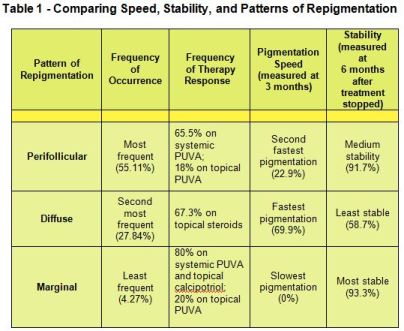
While the treatments used in this study were among the very best available at that time and are not necessarily those most often used today, the speed and stability of the repigmentation patterns reported are still relevant today.
Back to Top
What's On Your Mind?
Q. Is Green Tea Good for Vitiligo?
I've heard that Green Tea is good for vitiligo, but I've also heard that some of the other teas (like White Tea and Red Tea) are actually higher in antioxidants. What’s the difference, and is one better for vitiligo than the other?
- Over the years, tea has been ascribed many health benefits, including cancer and heart disease prevention, in addition to helping vitiligo. All tea comes from the same plant, Camellia sinensis; the difference between the various types lies in their processing and, in the case of white tea, the part of the plant it comes from (early leaves and buds). Tea contains polyphenols, plant chemicals that have been shown to reduce oxidative stress, which is found in the skin of those with vitiligo. Tea polyphenols include catechins such as EGCG, EGC, ECG, and EC, with green and white teas being the highest in EGCG, the most active catechin. Black tea is lowest in catechins because of the leaves are fully oxidized, while white and green teas are less processed. Green tea has anti-inflammatory, anti-oxidant, and immunomodulatory properties, all of which can be helpful to those with vitiligo.
 In the “Medical News Updates” section of this newsletter, we reported on a 2014 Chinese study of the benefits of EGCG on vitiligo in mice, showing that it decreased the time, area, and prevalence of depigmentation. The authors concluded that the administration of EGCG was “significantly associated with a decreased risk of vitiligo.” While white tea contains similar amounts of EGCG to the green tea studied, it isn’t studied as often because it is rarer and more expensive than green tea. In the “Medical News Updates” section of this newsletter, we reported on a 2014 Chinese study of the benefits of EGCG on vitiligo in mice, showing that it decreased the time, area, and prevalence of depigmentation. The authors concluded that the administration of EGCG was “significantly associated with a decreased risk of vitiligo.” While white tea contains similar amounts of EGCG to the green tea studied, it isn’t studied as often because it is rarer and more expensive than green tea.
How to increase the benefit: Interestingly, a 2007 study of the absorption rates of catechins by the body found that while minimal amounts of tea catechins were available when tea was consumed alone, however, adding juice, vitamin C, or milk seemed to protect the catechins from the digestive process, leaving more available to be absorbed. Lemon juice and rice milk increased catechin availability levels the most.
Hot, brewed teas contain more polyphenols than iced, instant, or ready-to-brew beverages, as polyphenol counts are affected by the type of tea, brewing time (longer is better), temperature (hotter is better), and the amount used.
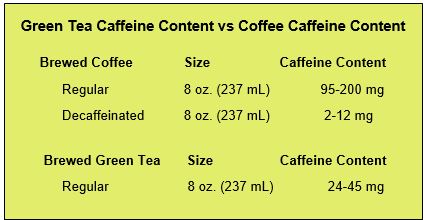
Decaffeination reduces the catechin levels by more than half, so to derive the greatest health benefit decaffeination is not recommended. The good news is, green tea is naturally low in caffeine with about 24-45 mg per 8 oz cup, and white tea with only 15-20 mg is even lower.
Organic: Recent studies show an increase in pesticide use among tea-growers, consequently, organic tea may be a safer option. All teas contain fluoride, so be cautious of the quantity you drink in areas where the water is also fluoridated. Also, loose tea leaves are thought to provide more benefits than bagged teas, partially because the water has better access to the leaves to extract the most catechins when the leaves aren’t as tightly packed, and partially because some commercial teabags may contain more crushed leaves and stems.
The teabag itself: Many teabags contain compounds that can leach chemicals into the finished teas, including paper teabags treated with epichlorohydrin, (a carcinogen that can also affect fertility and suppress immune function), and teabags made with synthetic polymers such as nylon, thermoplastic, PVC, and polypropylene.
For more information about teas made with toxin-free teabags: Click here.
Medical News Updates
Highlights of recently-published medical
articles on vitiligo and its treatments
A Future Test for Determining Vitiligo Susceptibility?

University of Arkansas investigators identified amino acid mutations, or changes, in genetic markers linked to vitiligo, reinforcing the concept that a genetic propensity exists for developing the disease. The animal study was published in August 2014 by a group of investigators that included Dr. Gisela Erf, a past speaker at VSI conferences. The project looked at the genome, or the complete set of an organism’s DNA, to pinpoint disease susceptibility. Identifying these genetic markers with amino acid mutations as being connected with the development of vitiligo could eventually lead not only to pinpointing the genetic basis for developing autoimmune vitiligo, but also to our ability to test for susceptibility to vitiligo in someone who does not have the disease, which would be a huge advancement.
Green Tea and Vitiligo
Could green tea help prevent vitiligo and treat the disease once it is established? A Chinese study published in August 2014 using mice, concluded that administering a key ingredient found in green tea epigallocatechin-3-gallate (EGCG), not only prevented onset of vitiligo in the mice that were studied, but in those with established disease, the substance decreased the prevalence of vitiligo lesions, the size of the areas of depigmentation, and the time before depigmentation developed. Drinking green tea certainly can’t hurt, but more studies are needed to prove a definitive benefit.
See additional information on green tea in the
“What’s On Your Mind” column in this newsletter.
Metabolic Syndrome
 Just in the last few years, a link between metabolic (biochemical processes that take place in the cells of your body’s organs, such as the liver, spleen, and pancreas) abnormalities and vitiligo has come to light. A 2014 study by several eastern European centers highlights the metabolic abnormalities that can occur in vitiligo. Dr. Pietrzak and colleagues looked at children with at least a six-month history of vitiligo lesions. They found that while the liver and spleen appeared normal in ultrasonographic scans, lipids and glucose tolerance were not normal. HDL-cholesterol (high density lipoprotein cholesterol) was much lower and LDL-cholesterol (low density lipoprotein cholesterol) was significantly higher in those with vitiligo compared to healthy controls. The same author first called our attention to the link between metabolic processes and vitiligo in a 2012 paper that discussed “metabolic syndrome” in vitiligo. This syndrome occurs in other inflammatory skin diseases, including psoriasis, and now growing evidence indicates similar abnormalities in vitiligo. Not only are lower HDL-cholesterol and higher LDL-cholesterol found in vitiligo patients, the ratio between the two appears increased, adding up to an increased risk for cardiovascular problems. These findings were found to occur in young vitiligo patients as well as adults. Just in the last few years, a link between metabolic (biochemical processes that take place in the cells of your body’s organs, such as the liver, spleen, and pancreas) abnormalities and vitiligo has come to light. A 2014 study by several eastern European centers highlights the metabolic abnormalities that can occur in vitiligo. Dr. Pietrzak and colleagues looked at children with at least a six-month history of vitiligo lesions. They found that while the liver and spleen appeared normal in ultrasonographic scans, lipids and glucose tolerance were not normal. HDL-cholesterol (high density lipoprotein cholesterol) was much lower and LDL-cholesterol (low density lipoprotein cholesterol) was significantly higher in those with vitiligo compared to healthy controls. The same author first called our attention to the link between metabolic processes and vitiligo in a 2012 paper that discussed “metabolic syndrome” in vitiligo. This syndrome occurs in other inflammatory skin diseases, including psoriasis, and now growing evidence indicates similar abnormalities in vitiligo. Not only are lower HDL-cholesterol and higher LDL-cholesterol found in vitiligo patients, the ratio between the two appears increased, adding up to an increased risk for cardiovascular problems. These findings were found to occur in young vitiligo patients as well as adults.
In addition to the cholesterol abnormalities mentioned above, vitiligo patients had an increased incidence of insulin resistance, diabetes, and high systolic blood pressure were found in a study by Dr. Karadag and colleagues in Turkey. Insulin resistance, even without the presence of diabetes, greatly increases the risk for cardiovascular problems. The study, published in 2011, looked at 57 vitiligo patients and 39 healthy controls of similar age and body mass index.
In a study published in 2012, the same authors found an additional link for cardiovascular risk in vitiligo patients: an increase in homocysteine, a common amino acid that has been connected to heart and vascular disease. Homocysteine also is associated with reduced levels of vitamin B12 and folic acid, and the investigators did find decreased levels of vitamin B12 in vitiligo patients. While this particular group did not identify lower folic acid levels, lower levels have been found in numerous other studies. Previous studies have confirmed the higher homocysteine levels in vitiligo patients, including one by Singh, et al that found higher homocysteine levels and identified the highest levels in those with active disease. Drs. Silverberg and Silverberg also confirmed the high levels of homocysteine as well as low levels of vitamin B12 in vitiligo patients.
One research group in Quebec, Canada found that the use of statins not only helped improve the lipid profile of a vitiligo patient but also led to regression of the patient’s vitiligo. This led the investigators to hypothesize that statins could be considered as a potential line of treatment for vitiligo and that the therapy’s success could be due to the fact that statins are immuno-modulators and vitiligo is an autoimmune disease. As mentioned in earlier VSI newsletters, John E. Harris, MD, PhD is conducting trials using the cholesterol drug simvastin in vitiligo patients at the University of Massachusetts Medical Center in Worcester, Massachusetts. VSI will let readers know when results are available.
Finally, new studies continue to show that many vitiligo patients tend to have low vitamin D levels, including two studies published this summer. The first study out of Turkey found that 48% of vitiligo patients studied had insufficient levels of vitamin D and 52% had very low levels. The second study out of Iran had similar findings. All vitiligo patients should get their vitamin D levels checked before taking over the counter vitamin D supplements, especially when using NB-UVB therapy, which has been shown to substantially increase vitamin D levels.
Autoimmune Thyroid - New Study Identifies
Autoantibodies Associated with White Hair
 An Italian study out this past summer found for the first time that in vitiligo patients, antibodies to Thyroid 3 (T3-Ab) were specifically associated with the appearance of white hairs, also known as leukotrichia. The study also found that antibodies to Thyroid 4 (T4-Ab) correlated with increased disease activity and duration in vitiligo. Astoundingly, the same study found that almost everyone with vitiligo – 97.5% -- had some kind of antibody against the thyroid. This exceptionally high figure for vitiligo patients contrasts greatly to the very low figure found in those who don't have vitiligo -- only 1 person out of 100 who did not have vitiligo had thyroid autoantibodies. The study examined 79 vitiligo patients and 100 controls (or people without vitiligo). VSI has frequently reported on the occurrence of autoimmune thyroid in vitiligo, but no studies to date have shown such high percentages of thyroid autoantibodies. An Italian study out this past summer found for the first time that in vitiligo patients, antibodies to Thyroid 3 (T3-Ab) were specifically associated with the appearance of white hairs, also known as leukotrichia. The study also found that antibodies to Thyroid 4 (T4-Ab) correlated with increased disease activity and duration in vitiligo. Astoundingly, the same study found that almost everyone with vitiligo – 97.5% -- had some kind of antibody against the thyroid. This exceptionally high figure for vitiligo patients contrasts greatly to the very low figure found in those who don't have vitiligo -- only 1 person out of 100 who did not have vitiligo had thyroid autoantibodies. The study examined 79 vitiligo patients and 100 controls (or people without vitiligo). VSI has frequently reported on the occurrence of autoimmune thyroid in vitiligo, but no studies to date have shown such high percentages of thyroid autoantibodies.
Another study from a research group in China also found significant evidence of autoimmune thyroid in vitiligo patients, although the percentages were lower at 23-24%. This group tested 87 vitiligo patients and compared them to 90 people who did not have vitiligo (matched by age and gender) and looked for thyroglobulin antibodies (TG-Ab) and thyroid peroxidase antibodies (TPO-Ab). An especially interesting aspect of this particular study was that the investigators also looked at risk according to gender and age and found that both females and teenagers with vitiligo were at the greatest risk of developing autoimmune thyroid disease than males or those with vitiligo of another age. Females with vitiligo had a 34.1% risk of developing autoimmune thyroid disease. Males of the same age had an 8.8% risk for antibodies to TPO-Ab and an 11.1% risk for antibodies to TG-Ab.
VSI stresses that all vitiligo patients – especially children, who often
are not routinely tested – should be tested for thyroid function and antibodies.
ReCell: Data Collection Wrapping Up
 ReCell, a device used for harvesting cells for transplantation in the outer layer of the skin (epidermis) of vitiligo patients, has been the focus of clinical trials in Austria over the last six years, and now investigators are collecting and analyzing the data. The trial is looking at the use of ReCell with and without narrow band UVB phototherapy and has focused on stable segmental vitiligo rather than the most common autoimmune-associated form, generalized vitiligo. Because the trial is in the data collection stage, patients are no longer being enrolled. ReCell, a device used for harvesting cells for transplantation in the outer layer of the skin (epidermis) of vitiligo patients, has been the focus of clinical trials in Austria over the last six years, and now investigators are collecting and analyzing the data. The trial is looking at the use of ReCell with and without narrow band UVB phototherapy and has focused on stable segmental vitiligo rather than the most common autoimmune-associated form, generalized vitiligo. Because the trial is in the data collection stage, patients are no longer being enrolled.
ReCell transplantation therapy is approved for use in Europe, Australia and China but not in the United States at this time. The proprietary device is supposed to reduce the very labor intensive cell separation process involved with the melanocyte keratinocyte transplant procedure (MKTP), which, if successful, would make the procedure much less complicated, resulting in wider availability of the treatment.
The trial, entitled "Epidermal Cell Transplantation in Vitiligo Skin With and Without Narrow-band Ultraviolet B (UVB) Treatment," started in 2008 at the Medical University of Graz in Austria. Investigators are looking at the percentage of repigmentation as the primary measure of success and also gauging the stability of the new pigment. VSI will let readers know the results of the trial as soon as the company that owns the rights to ReCell, Avita Medical, releases them.
SCENESSE® Phase 1 Trial Results Published
 Phase 1 clinical trial results are in for Scenesse® (afamelanotide), and so far the new therapy appears successful! The multi-center, randomized trial ran for a six-month period and involved 55 vitiligo patients, all of whom received NB-UV-B phototherapy and half who also received Scenesse® (afamelanotide) in addition to the phototherapy. Everyone had statistically significant improvement, but results for those who received the combination therapy were superior. Phase 1 clinical trial results are in for Scenesse® (afamelanotide), and so far the new therapy appears successful! The multi-center, randomized trial ran for a six-month period and involved 55 vitiligo patients, all of whom received NB-UV-B phototherapy and half who also received Scenesse® (afamelanotide) in addition to the phototherapy. Everyone had statistically significant improvement, but results for those who received the combination therapy were superior.
Scenesse® was administered via a subcutaneous dissolving implant about the size of a grain of rice. Repigmentation was determined by two scoring systems: the Vitiligo Area Scoring Index (VASI) and the Vitiligo European Task Force (VETF) score. Improvement for both groups of patients was seen early in the trial according to both scoring systems, but statistically significant improvement for the patients on the combination therapy came earlier and was more marked. By the end of the trial, those on Scenesse® plus phototherapy showed much greater improvement.
The combination therapy resulted in much greater repigmentation on the face and upper extremities, and results were seen, on average, 20 days earlier than in those on NB-UVB phototherapy alone. Both groups of patients generated both follicular (around the hair follicle) and peripheral (marginal) pigmentation patterns. The study did not test patients on Scenesse® alone, although the authors note that this should be studied in the future. The study also did not test the therapy in lighter-skinned patients, but in the darker-skinned patients who participated, results were most marked in those with the darkest skin.
Scenesse® acts similarly to a natural protein that is important in stimulating melanocyte production and proliferation. Clinuvel Pharmaceutical, the maker of Scenesse®, sponsored the study.
Back to Top
Research & Clinical Trials
New Needling Clinical Trial in New Jersey
Assessing the Efficacy of Needling
With or Without Corticosteroids in the Repigmentation of Vitiligo
Principal Investigator:
Babar Rao MD

Study Location:
Rutgers - Robert Wood Johnson Medical School
1 World’s Fair Dr, Somerset, NJ
Needling is an office-based procedure that transposes healthy, pigmented skin cells to depigmented areas using a needle. This trial will investigate the use of needling to treat vitiligo. It will compare needling alone to needling with corticosteroid.
Eligibility Requirements:
- Ages: 18 – 89 years
- Patients with 3 or more localized patches of stable vitiligo
- No prior treatment or had failed previous vitiligo treatments.
Exclusion Criteria:Those with the following will not be eligible:
- Unstable vitiligo (no new or changing lesions in past 6 months)
- Allergic to triamcinolone
- Using systemic treatments
- Pregnant
If you are interested in participating or would like more information:
Contact: Aida – 732-235-7765 or Danielle - [email protected] |
New Clinical Trial Opportunity in Italy
Efficacy of Autologous Outer-Root-Sheath
Melanocytes Transplantation in the Treatment of Vitiligo
Principal Investigator: Luigi Naldi MD

Study Location: Papa Giovanni XXIII Hospital, Bergamo, Italy
To determine whether the application of a non-cultured autologous hair
follicle outer-root-sheath melanocytes suspension, combined with targeted
UVB Phototherapy can lead to significant skin repigmentation in patients with stable vitiligo that were previously unresponsive to conventional treatments.
Eligibility Requirements:
- Ages: 18 – 60 years
- Presence of symmetric lesions of vitiligo at the back of the hands >5cm²
- Vitiligo lasting at least one year on the backs of both hands
- Stable vitiligo: no change for at least 6 months
- No systemic therapy, including PUVA, UVB phototherapy, or any anticoagulant drug, for at least two months prior to the enrollment date
- Suspension of topical medications for at least 15 days prior to the enrollment date
Exclusion Criteria:The following will not be eligible:
- Presence of active vitiligo or Koebner phenomenon
- Symmetrical areas of vitiligo on hands differing no more than 10% in size
- Presence of systemic infections or infections localized to the
tissues intended for transplantation
- History of infections to the tissues intended for transplantation (herpes simplex, human papillomavirus infections, pityriasis versicolor, pityriasis alba)
- Presence or history of malignancy
- Chemotherapy or radiation therapy in progress
- History of allergies or adverse reactions to local anesthetics
- Presence of transmissible diseases (HIV, hepatitis B and C,
human T-lymphotropic virus type I and II, syphilis, cytomegalovirus, Creutzfeldt-Jacob, tuberculosis)
- Women who are pregnant or intend to become pregnant during the study period (including breastfeeding women)
Treatment will consist of harvesting melanocytes from the outer-root
sheath of patient's hair follicles, then depositing in suspension (or saline
for placebo control) into abraded areas affected by vitiligo.
Afterward, patients will use targeted UVB phototherapy at home for
3 days / week from the beginning of the 5th week after transplantation
till the end of the study period (12th week).
If you are interested in participating or would like more information,
Simone Cazzaniga +39 035-2278 719 [email protected] |
Clinuvel Scenesse Clinical Trial
Opportunity in Singapore!
SCENESSE® Phase ll Clinical Trial
Study Location: National Skin Center, Singapore
The National Skin Centre is currently conducting research to assess a new
investigational study drug, afamelanotide (SCENESSE®) - a pigmentation
agent which may help to accelerate the repigmentation of the skin when used
together with the currently available therapy of Narrowband Ultraviolet B (NB-UVB) treatment. SCENESSE® is given in the form of an implant that slowly dissolves
in the body after administration under the skin.
Clinuvel Singapore Pte Ltd is seeking committed vitiligo patients
to participate in a 10-month trial at the National Skin Centre.
To participate in this clinical study,
individuals must meet the following criteria:
- at least 21 years of age
- nonsegmental vitiligo including the head and neck
- skin of mid to dark complexion
- no previous surgical treatment for vitiligo
- no light treatment (including NB-UVB phototherapy)
in the past 6 weeks
- no topical treatments (creams) for vitiligo in the past 4 weeks
- able to attend 10 study visits (around 2-3 hours) for 10 months
and come for NB-UVB twice a week for the first 7 months.
All study visits and NB-UVB treatments will
take place at the National Skin Centre.
Participants will be compensated for travel expenses. Study related
procedures and treatments part of the research will be given at no cost.
Your information will be kept confidential.
If you are interested in participating or would like more information:
Contact: Eric Wang Jun Yen
Phone: +65 90111867 or Email: [email protected] |
Melanocyte-Keratinocyte Transplant Procedure
Opportunity in Detroit!
Comparative Study Using Dermabrasion versus CO2 Laser
and Collagen Dressing versus Vaseline Gauze in MKTP
Principle Investigator: Iltefat Hamzavi, MD
Study Location:
Henry Ford Department of Dermatology,
3031 West Grand Boulevard Detroit, MI 48202
The melanocyte keratinocyte transplant procedure (MKTP) involves transplantation
of the skin cells that produce pigment from your normal skin to the depigmented skin. The procedure takes approximately 4 hours and is done under local anesthesia.
This is a prospective, open-label, parallel study comparing two different techniques
for preparing the depigmented skin (carbon dioxide laser versus dermabrasion)
and comparing two different wound dressings (collagen dressing versus vaseline impregnated gauze) for the melanocyte keratinocyte transplant procedure.
Eligibility Requirements:
- Must be 18 years of age or older
- Must have depigmented patches of skin
Exclusion Criteria:
- History of acral vitiligo (vitiligo on the hands or feet)
- Unstable vitiligo, defined as any new or enlarging areas of
depigmentation within the last 6 months)
- History of thickened scars or keloids
- History of koebnerization (getting new areas of
depigmentation at sites of trauma, such as a cut, scrape, or burn)
The vitiligo patch will be divided into four quadrants. Each quadrant will be
treated with the melanocyte keratinocyte transplant procedure, as follows:
- CO2 laser for denuding the epithelium Collagen dressing
- CO2 laser for denuding the epithelium Vaseline impregnated gauze dressing
- Dermabrasion for denuding the epithelium Collagen Dressing
- Dermabrasion for denuding the epithelium Vaseline impregnated gauze dressing
The patient will return to the clinic for the dressing removal 1 week post-procedure. Repigmentation of the treated areas will be assessed at 1 month, 3 months, and 6 months post-MKTP.
To participate, or for more information,
Contact: Dr. James L. Griffith
Phone: 313-916-6964 or Email: [email protected] |
Your Opportunity to Move Research Forward!
University of Colorado
Health School of Medicine
International Study to Find Vitiligo Genes
Update!
Additional Patient Volunteers Needed
From the
USA and Canada
Scientists with the International VitGene Consortium project spanning 18 countries are working to understand the biology of vitiligo so that more effective vitiligo treatments can be designed.
Thanks to your involvement, the first two phases of this research project have been extraordinarily successful, discovering many vitiligo genes, and resulting in real breakthroughs in understanding and opening doors to potential new treatments.
The U.S. National Institutes of Health (NIH) has now awarded a large research grant for a third phase of these studies, to discover additional vitiligo genes, deepen understanding, and provide even more new targets for vitiligo treatment. To accomplish this, they need to enroll 3000 additional Caucasian (white) vitiligo patients over the next two years. Participants must be from the USA or Canada and not have previously taken part.
Your participation is vitally needed. Please complete the questionnaire below and then email directly to Dr. Richard Spritz at the University of Colorado School of Medicine using the email address provided at the end of the questionnaire.
Your personal information, by law,
will be kept private and will not be sold or disclosed.
Join with us to work for a vitiligo-free future!
|
NEW! - Support VSI Through Ebay
New Way To Support VSI Through Ebay!
Do you sell items on eBay, or want to hold an online garage sale? If so, consider donating a percentage of your proceeds to VSI through eBay’s Giving Works program! It’s easy – when you list an item through a Giving Works listing, choose to send 10-100% of the final sale price to VSI. Your listing will have a special placement and designation. You’ll receive a proportional fee credit from eBay, and will also receive a tax donation receipt when the donation is deducted from your funds received. It’s a great opportunity to make some money for yourself and for VSI, so clean out those closets and garages and get selling!
To Learn More About VSI's Giving Works: Click here |
Earn Funding for VSI 3 Ways When You Shop!
Please keep VSI in mind when you do any of your online shopping
AMAZON SHOPPING
Amazon.com has all kinds of items in addition to books. As long as shopping is done through this link, Amazon.com, or from the Amazon box on our Community Home Page, VSI will earn fees, based on a percentage of the sale*. The more items members buy, the higher the percentage! Our Vitiligo Library and Store, containing books, articles and products for those with vitiligo, is also powered by Amazon.
iGIVE SHOPPING
iGive.com is another program with an online shopping mall with over 700 stores where you can shop and earn VSI a percentage-coupons are often available as well.
Let friends and family know about iGive so they can support VSI, too. You do have to register for iGive. Once you've registered, you can either shop directly through their "mall" on iGive's website or by downloading their new button, which makes it even easier. iGive also has a search function powered by Yahoo at isearchigive.com (or through the button) that earns VSI a penny per search. The power of numbers makes this also an effective way to support VSI.
GOODSEARCH SHOPPING AND DINING!
GoodSearch and Goodshop are similar to iGive; click “get started” and designate Vitiligo Support International as your cause - you can also register, or sign in through Facebook, to keep track of your donations (registration is not required). Goodshop has some different stores (like Target), though, and also offers coupons and often a higher percentage to VSI. Goodsearch also offers an optional toolbar. Through GoodDining, participating restaurants automatically donate a percentage of your meal purchases to VSI if you (securely) register your credit cards. If you provide reviews of the restaurants afterwards, we earn even more!
* Vitiligo Support International Inc., (VSI) is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. |
|

