For very best viewing, Click Here: Winter Newsletter |
 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
This Newsletter Has Been Generously Sponsored By:

Click Above for More Information on Home Phototherapeutic Light Units for Vitiligo
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|

Dear Members and Friends of VSI, Vitamin D is a growing focus of research interest. A wide variety of diseases, such as cardiac disease, neurological disorders, autoimmune disease, and various cancers, are now being studied for a possible link to vitamin D insufficiency. Conflicting opinions and data on the effectiveness of supplementing with vitamin D/maintaining higher base levels of vitamin D to combat these conditions have made it difficult for the average person to know what to do. In 2010, the National Academy of Sciences Institute of Medicine (IOM) issued revised dietary and testing guidelines concerning how to maintain a healthy level of vitamin D. So why is this important for people with vitiligo? According to preliminary research, having low blood levels of vitamin D may trigger vitiligo, an autoimmune disease, as well as secondary autoimmune disease in vitiligo patients. A US study found that many vitiligo patients had low levels of vitamin D as well as a greater risk of secondary autoimmune diseases like Hashimoto thyroiditis, lupus and others. A Chinese researcher has just reported that the dysfunction of the vitamin D receptor (VDR) gene may be involved in the cause of vitiligo. This research, and what it means for vitiligo patients, is summarized in this issue. The pace of research has quickened and technology continues to improve. VSI will be meeting with vitiligo researchers from the United States and around the world this year to discuss avenues of promising research and how VSI can help. We encounter many opportunities to collaborate with medical, research and commercial interests as a result of our hard work. We can see a very promising future, but we can't reach it without increased funding. We rely on the support of a few, but we need the support of many more who care about vitiligo research and awareness. If you find the newsletter helpful, you feel vitiligo research is important, and you want a national organization like VSI to speak out on your behalf, your gift today will help us continue this work. Sincerely,
Jackie Gardner
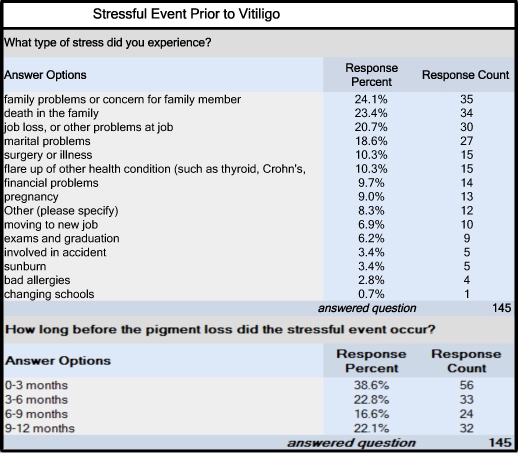
New Survey!
Vitamin D insufficiency may be a factor in triggering vitiligo according to recent research. This finding is consistent with the current belief of many researchers that vitamin D, in addition to maintaining bone strength, may also have a role in maintaining the health of various organs and systems. A wide variety of diseases, such as cardiac disease, neurological disorders, autoimmune disease, and various cancers, are now being studied for a possible link to vitamin D insufficiency. While more research is needed to better understand these links, it is important that everyone with vitiligo be aware that maintaining healthy levels of vitamin D may prove helpful in managing vitiligo as well as in protecting against secondary disease. What is vitamin D and how do we get it? Vitamin D is actually a hormone predominantly generated by the action of ultraviolet light on the skin. Since one of its primary functions is to maintain normal production levels of calcium and phosphorus, it is most well-known for helping to form and maintain strong bones. More recently, certain autoimmune disorders (including vitiligo) have been linked to low vitamin D levels, which may be due to vitamin D's anti-inflammatory and immune-modulating properties.
Interestingly, researchers have found that exposing mushrooms, already a natural source of vitamin D, to either sunlight or UVB light can dramatically boost their vitamin D levels. UV-exposed mushrooms are available in some stores, but the research showed that the vitamin D levels of any mushrooms can be boosted by sunlight, even with only a couple of hours of exposure. The increased levels of vitamin Is there a link between vitamin D and vitiligo? Recent studies have pointed to a possible connection between vitiligo and vitamin D levels. One study of a village in Romania found many families with vitiligo and other autoimmune diseases who also had a genetic abnormality in a vitamin D receptor (VDR) gene. A similar genetic abnormality in the VDR gene was found by Chinese investigators in 749 patients with vitiligo, adding additional evidence of a connection between this gene and vitiligo. A 2010 US study also found evidence of a potential vitamin D linkage. A majority of vitiligo patients were found to have low to very low levels of vitamin D. Also, in this group, over 13% had secondary autoimmune disease. The study authors concluded that very low vitamin D levels would be a good screening criteria for the presence of additional autoimmune disease in vitiligo patients. How much vitamin D do I need? The necessary amount of daily sunlight one needs to synthesize a sufficient level of vitamin D varies with age, skin type, season, latitude, time of day, etc. During periods of sunlight, vitamin D is stored in body fat and then released when sunlight is gone. If one cannot get enough sun exposure, vitamin D supplements (vitamin D3/cholecalciferol) can provide an alternate source. Short-term treatment of vitamin D deficiency may require doses of vitamin D that exceed the IOM’s recommended maximum amount of 4,000 IUs. People with certain conditions, such as primary parahyperthyroidism, sarcoidosis, the presence of kidney stones, unexplained hypercalcemia, renal insufficiency or kidney failure, or people at risk for vitamin D deficiency, should use vitamin D supplements only under the guidance of a physician. Assuming minimal sun exposure, the IOM recommends the daily dietary vitamin D intake (food or in combination with supplements) shown below.
If one gets midday sun exposure during warmer months and regularly consumes foods rich in vitamin D, supplements most likely are not needed. People who have the risk factors discussed below might need supplements, though the amount in most multivitamins may be enough. Who is at greater risk for low levels of vitamin D? Factors that increase the risk for vitamin D deficiency include:
The sun’s rays are strongest at the equator, where the sun is most directly overhead and UV rays must travel the least distance. At higher latitudes, because the sun is lower in the sky, UV rays must travel a greater distance through ozone-rich portions of the atmosphere and are less intense as a result. What Happens if You Take Too Much Vitamin D? People can experience side effects from vitamin D if they take too much over an extended period of time. The side effects typically relate to levels of calcium that have become too high because calcium absorption works in synergy with vitamin D. Side effects from excessive levels of vitamin D include weakness, fatigue, sleepiness, headache, loss of appetite, dry mouth, nausea, and vomiting.Medication Interactions
Drugs that can increase calcium levels when vitamin D is taken: Digoxin (Lanoxin) This medication treats irregular heart rhythms. Vitamin D supplement may cause levels of calcium to get too high in the blood. Calcipotriene (Dovonex) This is a vitamin D3 based topical medication prescribed for psoriasis and vitiligo. Taking an additional vitamin D supplement when using this topical prescription could cause calcium levels to get dangerously high in the blood. Drugs made less effective by vitamin D: Atorvastatin (Lipitor) Taking vitamin D may reduce the amount of Lipitor absorbed by the body, making it less effective. Anyone taking a statin, or cholesterol-lowering drug, should discuss vitamin D supplementation with his/her physician. Calcium channel blockers Vitamin D supplements may interfere with the effectiveness of high blood pressure and heart condition medications. Examples of these drugs are: nifedipine (Procardia); verapamil (Calan); nicardipine (Cardene); DitiaZem (Cardizem, Dilacor); and amlodipine (Norvasc). Diltiazem (Cardizem, Dilacor, Tiazac) These drugs are used to manage chronic stable angina and angina due to coronary artery spasm. Vitamin D helps the body absorb calcium. Calcium can affect the heart. Taking a large amount of vitamin D may decrease diltiazem’s effectiveness. Vitamin D may increase how quickly the liver breaks down these medications, decreasing their effectiveness
Drugs that may increase vitamin D blood levels: Estrogen: This hormone raises vitamin D levels in the blood, which may promote calcium and bone strength. Also, taking vitamin D supplements along with estrogen replacement therapy (ERT) increases bone mass more than ERT alone. This may not be true if you are taking progesterone. Isoniazid (INH): a medication used to treat tuberculosis Diuretics: Reduce an accumulation of fluid in your body. As a result, they can increase vitamin D activity and lead to high levels of calcium in the blood.
Drugs that may lower vitamin D blood levels: Antacids: Long-term use of antacids may change the levels, metabolism, and availability of vitamin D. Anti-seizure medications: Corticosteroids (prednisone) Long-term use of corticosteroids can cause bone loss. Supplements of calcium and vitamin D can maintain bone health. Supplements may be especially important in this case. Bile acid sequestrants taken to lower cholesterol, such as cholestyramine (Questran, Prevalite) and cholestipol (Colestid) Rifampin: Used to treat tuberculosis. Mineral oil: Interferes with vitamin D absorption Weight-loss drugs: orlistat (Alli, Xenical) Prevents body from absorbing fat. May prevent absorption of fat-soluble vitamins such as vitamin D. Orlistat patients are often prescribed a multivitamin along with fat-soluble vitamins. How do I know if I have a sufficient level of vitamin D? Even with the recommendations of the IOM, there is no scientific consensus on the appropriate amount of vitamin D the average person should take. Some scientists feel that the dietary intake levels should be much higher, up to 10,000 units or more. However, in the words of one of the authors of the IOM guidelines, JoAnn Manson, PhD, MD, “It is our opinion that vitamin D deficiency is not as widespread as reported because laboratories across the country are using different cut points that overestimate the number of people with vitamin D deficiency.” Controversy over Supplements Not all scientists agree that increasing vitamin D levels is helpful, either in cancer prevention or even in preventing fractures, previously thought to be its main purpose. Others are adamant that maintaining a healthy level of vitamin D increases lifespan and decreases the risk of several cancers, along with strengthening bones, of vital interest to the elderly who are at risk of falls and fractures. Since studies can be found to support either side, there’s plenty of room for disagreement. Studies Urging Caution A government panel recently recommended against the daily use of vitamin D supplements by healthy, post-menopausal women. It said the science is not sufficiently developed to claim any benefits from vitamin D supplements for this group of women and the science, in fact, was still out for pre-menopausal women and women, stating that studies examining vitamin D’s role in reducing cancer risk were mixed, and therefore inconclusive. While it did find that supplementing with vitamin D and calcium decreased the risk of falls in the elderly, it was unsure of their benefits in preventing fractures.There is also concern that people might take too much vitamin D, raising their levels too high. A group in Copenhagen reviewed blood sample results from almost 250,000 Copenhageners (Denmark has a civil registration system that makes these studies possible) and found that, while low levels of vitamin D increase mortality, so do high levels over 140 nanomoles per liter. While they were unsure of the reason for the increase in mortality at higher levels of vitamin D, they said that it may cast doubt on the ‘more is better’ crowd, and that more research is needed in this area. Studies Supporting Supplementation In 2010, a team led by Dr. Joan Lappe from Creighton University published results of a study on 1,179 healthy postmenopausal women. The women were randomly assigned daily doses of calcium alone, calcium plus vitamin D, or placebos. After four years, they found that while both groups taking supplements had a dramatically lower risk of developing cancer, the risk was even lower in the group that took vitamin D as well. The study also showed that the higher the blood level of vitamin D, the lower the cancer risk. This study led the Canadian Cancer Society to recommend that all adult Canadians take a daily supplement of 1,000 IU to minimize cancer risk (Canada’s latitude places them at higher risk of deficiency). According to Dr. Lappe, “it’s inexpensive, it’s safe, and it’s easy to take. It’s something that should be considered by a lot of people. It’s low-risk with maybe a high pay-off.” Also in 2010, a research team from Oxford University in England found significant links between vitamin D receptors, which control how the genes use vitamin D, and genetic regions associated with several autoimmune diseases, including multiple sclerosis, Crohn’s disease, and type 1 diabetes (diseases also sharing genes with vitiligo), and also regions associated with some types of cancer. They noted that vitamin D might play a role in a vast variety of biological processes. The lead investigator said their findings indicated that vitamin D was involved with the development of these diseases and that there could be serious risks from vitamin D insufficiency, especially in those genetically prone to be deficient. He went on to say, “Considerations of vitamin D supplementation as a preventative measure for these diseases are strongly warranted.” What should a person with vitiligo do? Deficiency in vitamin D has been widely regarded by researchers as a possible environmental trigger for many autoimmune diseases, theorizing vitamin D deficiency could not only trigger the onset of an autoimmune disorder, but also cause the disease to worsen. Though more research is needed to understand the nature of this linkage, people with vitiligo should discuss with their physician the possible benefits of maintaining adequate levels of vitamin D as part of managing their vitiligo as well as to screen for the development of other autoimmune disorders.
The American Academy of Dermatology (AAD) is celebrating the 20th Anniversary of Camp Discovery with six weeks of Camp in five states; providing an amazing camp experience to approximately 350 children each year. There is no fee to attend; full scholarships, including transportation, are provided by the AAD through generous donations from its members, outside organizations and individuals. All campers must be referred by their dermatologist. 2013 Dates:
Referral forms are available now, and the application deadline is April 15, 2013. For more information about attending or volunteering, please visit the Camp website at www.campdiscovery.org, or contact Janine Mueller at 847- 240-1737, or by email: [email protected]
What's On Your Mind? Q. Since people with vitiligo tend to lose skin pigment in patches, does the hair growing out of these patches also lose pigment?
Q. Does starting treatment right away when my vitiligo starts spreading make any difference?
Highlights of recently-published medical Preliminary Scenesse: First Phase Results Look Promising According to Clinuvel, the company that manufactures Scenesse, 41 out of 54 patients with vitiligo completed the trial; 13 patients dropped out due to their inability to conform to the challenging treatment protocol and five due to the intensity of pigmentation. All were reported to have experienced no serious side effects and to tolerate the drug well. The participants were split equally into two groups on a random basis: one receiving combination therapy, the other monotherapy. The combination therapy group was treated 3 times weekly with NB-UVB and, starting in the second month, received a series of 4 monthly implants containing afamelanotide followed by a final month of NB-UVB monotherapy. The monotherapy group of patients was treated with NV-UVB alone over the 6 month study period. The results showed that first signs of repigmentation occurred earlier in those on the combination therapy, (median 43 days versus 68 days) and those with the darkest skin complexion achieved a deeper and more complete repigmentation compared to those only being treated with NB-UVB. The participants will continue being followed for up to six months to monitor the stability of the repigmentation as well as to identify any new pigment loss. In the words of the Clinuvel Chief Scientific Officer Dr. Dennis Wright, “The clinical significance of these observations from CUV102 is most promising. The proposed combination therapy with Scenesse enables a faster and more complete repigmentation for people with vitiligo. This has the potential to substantially reduce the current regimen of 18 months of NV-UVB treatment thrice per week…” At this time, Clinuvel is considering a "Phase IIb" vitiligo study. After completing regulatory filings and approvals, this study phase would likely begin in Europe and Asia. Barring any unforeseen complications, they predict a "best case scenario" of 2 to 3 years before the product will be available around the world for vitiligo. Scenesse is a linear peptide that can activate production of melanin in the skin. A physician implants it underneath the skin in the fatty area of the hip as a dissolvable implant approximately the size of a grain of rice. In the normal skin, the effects become visible approximately 2 days later as the skin darkens due to the activation of the melanin in the skin. Clinuvel Pharmaceuticals is an Australian biopharmaceutical company focused on developing drugs for the treatment of a range of severe skin disorders. Clinuvel reports that Scenesse is available by physician’s prescription in Italy and Switzerland for treatment of erythropoietic protoporphyria (EPP) only; not for vitiligo. Editor’s Note: VSI would like to thank Clinuvel for their dedicated communication with VSI during this phase of the study. Their consistent briefings and updates enabled VSI to in turn keep the vitiligo community informed of the ongoing progress. We look forward to helping facilitate (the conduct) of future phases of this promising therapy.
Study of Vitiligo Patients Finds Melanoma And Recent genetic studies have suggested that patients with vitiligo face a lower risk from melanoma cancer. They point to autoimmunity in patients with vitiligo which may protect against melanoma development. On the other hand, in theory, the lack of protective melanin may lead to more photodamage and an increased risk of melanoma and nonmelanoma skin cancer (NMSC). Some doctors are hesitant to prescribe phototherapy or recommend sun exposure because of this potential risk. But are vitiligo patients really at risk? Dutch researchers reporting in the British Journal of Dermatology retrospectively assessed the actual incidence of melanoma and nonmelanoma skin cancer (NMSC) of vitiligo patients against controls. The researchers analyzed 1307 mailed surveys returned by patients with nonsegmental vitiligo, who were at least 50 years old. The questions they were asked related to demographics, vitiligo characteristics, phototherapy history, skin cancer risk factors and the number of skin cancers experienced during the patient’s lifetime. Patients were asked to have a spouse or friend in the same age group fill out the questionnaire as a control; 708 controls without vitiligo responded. Skin cancers reported were confirmed by a pathology report. Reported results from controls were in line with population norms. They found that patients with vitiligo had fewer melanomas and NMSC than the controls. They were three times less likely to develop any skin cancers than the control group even when known skin cancer risk factors such as childhood sunburn and high mole count were considered. They also found that vitiligo patients treated with phototherapy did not experience increased rates of skin cancers, even those phototherapy patients who received more than 300 treatments. The Dutch investigators suggested that the decreased risk of melanoma in vitiligo patients might be due to the anti-melanocyte autoimmunity, and is also consistent with recent studies finding that melanoma and vitiligo are genetically incompatible. They speculated that the lower rate of NMSC may be due to the decreased photodamage and the increased levels of wild-type p53 expression they observed in the keratinocytes in the skin of vitiligo patients. As p53 is a tumor suppressor protein that protects again cancer, it may protect those with vitiligo from actinic damage and keratinocyte cancer. In summary, authors of this study, the largest of its type, concluded that patients with vitiligo are far less likely to develop melanoma and NMSC over their lifetimes than the average population, and indicate that the risk is not increased by phototherapy. They recommend prospective studies in different populations to corroborate these results.
Vitamin D Deficiency May Play Role In Vitiligo
Dr. Nanette Silverberg, Director of Pediatric Dermatology at St. Luke’s-Roosevelt Hospital Center and Beth Israel Medical Center, and colleagues set up a pilot study of 45 vitiligo patients, ages 2-71, to find out if there was an association between vitiligo and low vitamin D levels. None of the patients took vitamin D supplements, and were estimated to receive at most 200 IU per day from food sources. Sunscreen use (which can affect the body’s production of vitamin D from sunlight) was not considered. Of the 45 patients, 13.3 percent were found to have very low vitamin D levels (<15 ng/mL) and a greater chance of having a second autoimmune disease, including autoimmune thyroid disease (Hashimoto’s thyroiditis and Graves’ disease), lupus, alopecia areata, and inflammatory bowel disease; overall, one-third of the study group had another autoimmune disease in addition to vitiligo. Dr. Silverberg suggested very low vitamin D levels might be a good screening tool for the presence of additional autoimmune illness in vitiligo patients. Dr. Silverberg and her colleagues also found that the frequency of lower vitamin D levels increased with the age of the patient; low levels were observed beginning at age 3 and decreased over time. The researchers observed that the decrease in levels as patients age may contribute to the development of secondary autoimmune disease. The researchers identified the need to explore the relationship between vitamin D receptors (that are involved in a variety of biological processes, including those related to pigment formation) and vitiligo disease activity; whether increased vitamin D intake may prevent vitiligo or related autoimmune conditions in family members of vitiligo patients who may share similar genetic predisposition; and the possibility that supplementation with vitamin D might help control long-term disease activity in vitiligo.
Vitamin D Gene May Trigger Vitiligo In Chinese Individuals Chinese researchers at the Fourth Military Medical University in Xi’an, China report in the British Journal of Dermatology that the vitamin D receptor (VDR) gene may be associated with vitiligo. These researchers suggest that this gene, which affects vitamin D production, may not be functioning normally in people with vitiligo and may be a factor for susceptibility of vitiligo. They hypothesized that gene variations might be the reason for this dysfunction.
They discovered that several specific VDR variations among these four alleles were found more often in the control group and were associated with a lower risk of vitiligo. Two of these same variations were mentioned as also relating to higher levels of vitamin D when compared to the variations found more often in those with vitiligo, seeming to show a connection between increased vitamin D levels and decreased risk of vitiligo. Higher levels (above 18.72 ng/mL) of vitamin D were associated with a significantly lower risk for vitiligo, and the risk increased with levels below 14.95 ng/mL. The researchers said that the results suggest that VDR variations do appear to affect VDR function and vitamin D levels, and could identify those with a predisposition to vitiligo in the Chinese population.
Clinical Trial in Massachusetts!
Major Expansion of Vitiligo Genetics Project
Patients and Controls Invited to
Earn Funding for VSI 3 Ways When You Shop! Please keep VSI in mind when you do any of your online shopping
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Copyright © 2013 Vitiligo Support International Inc. All rights reserved. Reproduction or republication strictly prohibited without prior written permission A Vitiligo Support International, Inc. financial statement is available upon written request from the Virginia Office of Consumer Affairs. Mail requests to: Virginia Department of Agriculture and Consumer Services, Office of Consumer Affairs, P.O. Box 1163, Richmond, Virginia 23218. Click here to unsubscribe |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 Vitamin D has several forms, but the form of greatest importance is vitamin D3 (also known as cholecalciferol), which is synthesized in the skin when it is exposed to sunlight. Sunlight is the greatest source of vitamin D for humans. Historically, about 90% of our required vitamin D was synthesized from the effects of UVB rays on the skin. The remaining 10% came from the few foods in nature which contain vitamin D. Cod and fish oils and fatty fish such as salmon, tuna, sardines and mackerel are among the best sources. Beef liver, cheese, egg yolks and mushrooms provide small amounts.
Vitamin D has several forms, but the form of greatest importance is vitamin D3 (also known as cholecalciferol), which is synthesized in the skin when it is exposed to sunlight. Sunlight is the greatest source of vitamin D for humans. Historically, about 90% of our required vitamin D was synthesized from the effects of UVB rays on the skin. The remaining 10% came from the few foods in nature which contain vitamin D. Cod and fish oils and fatty fish such as salmon, tuna, sardines and mackerel are among the best sources. Beef liver, cheese, egg yolks and mushrooms provide small amounts. 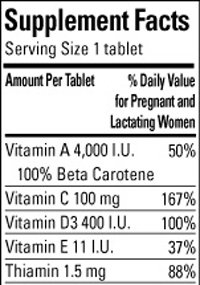 Today, we have less overall exposure to sunlight. Despite this, however, the availability of supplements, multivitamins and foods fortified with vitamin D has helped most Americans maintain adequate levels of vitamin D according to the National Academy of Sciences, Institute of Medicine (IOM), which sets the national standards for intake of vitamins and other nutrients. Almost all of the U.S. milk supply is fortified with vitamin D, as are many breakfast cereals and some brands of orange juice, yogurt, margarine, and soy beverages.
Today, we have less overall exposure to sunlight. Despite this, however, the availability of supplements, multivitamins and foods fortified with vitamin D has helped most Americans maintain adequate levels of vitamin D according to the National Academy of Sciences, Institute of Medicine (IOM), which sets the national standards for intake of vitamins and other nutrients. Almost all of the U.S. milk supply is fortified with vitamin D, as are many breakfast cereals and some brands of orange juice, yogurt, margarine, and soy beverages. D produced were long-lasting even when the mushrooms were cooked or dried, without any loss in vitamin content. A German study found that vitamin D levels were comparable between those who took supplements and those who ate UV-enhanced mushrooms. Some mushrooms are very high in tyrosine, an amino acid involved in pigment production. An Iranian study also showed that one of the components of mushrooms, tyrosinase, inhibited vitiligo in mice, and surmised that consuming mushroom tyrosinase may be of benefit to those with vitiligo. Since some mushrooms also stimulate the immune system, which some recommend avoiding with autoimmune disease, you should first discuss adding an abundance of mushrooms to your diet, with your doctor.
D produced were long-lasting even when the mushrooms were cooked or dried, without any loss in vitamin content. A German study found that vitamin D levels were comparable between those who took supplements and those who ate UV-enhanced mushrooms. Some mushrooms are very high in tyrosine, an amino acid involved in pigment production. An Iranian study also showed that one of the components of mushrooms, tyrosinase, inhibited vitiligo in mice, and surmised that consuming mushroom tyrosinase may be of benefit to those with vitiligo. Since some mushrooms also stimulate the immune system, which some recommend avoiding with autoimmune disease, you should first discuss adding an abundance of mushrooms to your diet, with your doctor.

 The IOM defines vitamin D deficiency as anything below a minimum blood level of 30 nanograms per milliliter of blood (ng/ml) and an optimal blood level of 50 ng/ml. A simple blood test called "25-hydroxyvitamin D," also called 25(OH)D (includes the sum of vitamin D2 and vitamin D3), will provide your vitamin D level and is the only way to confirm that you are getting an adequate amount of vitamin D. Many physicians automatically conduct the test on high-risk groups (including people who are overweight, 50 and over, etc.), but you can always ask your physician for the test. If the results of your test are abnormal or unexpected, you should discuss them with your physician.
The IOM defines vitamin D deficiency as anything below a minimum blood level of 30 nanograms per milliliter of blood (ng/ml) and an optimal blood level of 50 ng/ml. A simple blood test called "25-hydroxyvitamin D," also called 25(OH)D (includes the sum of vitamin D2 and vitamin D3), will provide your vitamin D level and is the only way to confirm that you are getting an adequate amount of vitamin D. Many physicians automatically conduct the test on high-risk groups (including people who are overweight, 50 and over, etc.), but you can always ask your physician for the test. If the results of your test are abnormal or unexpected, you should discuss them with your physician. Researchers at McGill University in Canada have just published a study showing that the active form of vitamin D works to slow down progression from pre-malignant cells to malignancy, and may also slow down the reproduction of cancerous cells. One of the authors, Dr. John White, stated, “We hope that our research will encourage people to maintain adequate vitamin D supplementation and will stimulate the development of large, well-controlled cancer chemoprevention trials to test the effects of adequate supplementation.”
Researchers at McGill University in Canada have just published a study showing that the active form of vitamin D works to slow down progression from pre-malignant cells to malignancy, and may also slow down the reproduction of cancerous cells. One of the authors, Dr. John White, stated, “We hope that our research will encourage people to maintain adequate vitamin D supplementation and will stimulate the development of large, well-controlled cancer chemoprevention trials to test the effects of adequate supplementation.”

 Scenesse (known generically as afamelanotide) is a brand name drug being tested in combination with narrowband UVB (NB-UVB) in treating vitiligo. The hope is that Scenesse® will accelerate narrowband’s ability to repigment vitiligo. Recently-released results of a six-month, Phase IIa US trial of the drug seem to confirm this outcome.
Scenesse (known generically as afamelanotide) is a brand name drug being tested in combination with narrowband UVB (NB-UVB) in treating vitiligo. The hope is that Scenesse® will accelerate narrowband’s ability to repigment vitiligo. Recently-released results of a six-month, Phase IIa US trial of the drug seem to confirm this outcome. Many autoimmune diseases such as rheumatoid arthritis, type 1 diabetes, and multiple sclerosis, have been associated with reduced vitamin D levels. Vitiligo is also an autoimmune disease that is also associated with other systemic autoimmune diseases including hypothyroidism and hyperthyroidism, adult-onset type 1 diabetes, and systemic lupus erythematosus. However, it is unknown whether vitiligo and its occurrence with other systemic autoimmune conditions is a result of reduced vitamin D levels.
Many autoimmune diseases such as rheumatoid arthritis, type 1 diabetes, and multiple sclerosis, have been associated with reduced vitamin D levels. Vitiligo is also an autoimmune disease that is also associated with other systemic autoimmune diseases including hypothyroidism and hyperthyroidism, adult-onset type 1 diabetes, and systemic lupus erythematosus. However, it is unknown whether vitiligo and its occurrence with other systemic autoimmune conditions is a result of reduced vitamin D levels. The objective of the researchers was to identify and evaluate any association between certain VDR gene variations and vitamin D levels in those with vitiligo compared to a control group. They performed a hospital-based study of 749 patients with vitiligo and 763 matched controls, looking at four VDR gene alleles (one of 2 or more forms of a gene) and vitamin D levels to determine whether they were associated with vitiligo risk in the Chinese population.
The objective of the researchers was to identify and evaluate any association between certain VDR gene variations and vitamin D levels in those with vitiligo compared to a control group. They performed a hospital-based study of 749 patients with vitiligo and 763 matched controls, looking at four VDR gene alleles (one of 2 or more forms of a gene) and vitamin D levels to determine whether they were associated with vitiligo risk in the Chinese population.