

Message From the How Do I Treat my Vitiligo
Sunscreens: Pros,
Earn funding for VSI View Past Newsletter Issues
VSI Medical and Scientific For more information on
VSI's MSAC Click Here |
|
Having trouble remembering your Logon ID or Password? Beneath the login field on the Community Page you'll find instructions to have them sent to you.
|
Online Email Contact Us Postal Mail Address Phone |
|
VSI wishes to express our deepest sympathy to the people of Japan and all those whose lives have been affected by the earthquake and tsunami. |
 |
Dear Members and Friends of VSI,
Frustrated with medical therapy? If you are among the group of vitiligo patients for whom medical therapy has not worked, you may be thinking about whether surgery or depigmentation is for you. Surgery can be effective and depigmentation has been a successful choice for many. Both, however, require patience and commitment and work better for some than others. So what should you know?
In this Spring issue of our newsletter, we highlight what science has reported as to the ultimate benefit of these therapies. This is the second of a two-part series on vitiligo treatment. In our Winter issue, we reviewed the traditional medical therapies available for vitiligo, which are effective for the majority of people. However, for those whom medical therapy is of limited or no value, surgery and depigmentation are options.
Consulting with an informed dermatologist and talking with others who have had surgery or depigmentation are additional critical steps to becoming informed. The more you know, the easier the decision will be for you. Visit VSI's forums on our web site to see what others have said about their therapeutic experience, which can help you become better informed.
For all of you looking forward to the summer yet wanting to protect your skin from the sun, read our updates on sunscreens in this issue. Though sunlight can be therapeutic for vitiligo, we all need to be prudent in how much we expose ourselves to the sun's rays. We also know many are concerned about the safety of sunscreens so we have reviewed what is known (and not known) about sunscreen chemicals.
Call or write us if we can help.
Sincerely,

Jackie Gardner
|
Please consider a donation to VSI. Our newsletter service is supported entirely by donations. VSI's mission of education and advocacy is enabled by the generous support of the vitiligo community and its partners. With your donation, you will be supporting the only comprehensive reporting on scientific and medical events in vitiligo for the public. You can make your gift today by clicking here. |
How Do I Treat My Vitiligo
A Review of Treatment Choices - Part II
Depigmentation & Surgical Options
|
We focus on surgery and depigmentation in this issue as part of our second in a series featuring the medical therapies for vitiligo. In our Winter 2010 issue, we featured the first-line medical therapies used to treat localized and extensive vitiligo. The depigmentation and surgical procedures featured here are generally second-line strategies for those who have not had satisfactory results from medical therapy. |
Depigmentation: To Pursue or Not to Pursue
If you have vitiligo, you most likely have heard of depigmentation, the process by which the remaining pigment is permanently removed from the skin and wondered where it fits into vitiligo treatment. Is it something you should consider?
People who consider depigmentation have reached a point where medical therapy no longer offers hope for controlling their disease. Generally, the vitiligo has become so severe that one has come to the place where you either continue to live with the diseases progression or depigment. Some who have extensive vitiligo find it preferable, and easier, to depigment the remaining unaffected skin rather than try to repigment the vitiligo-affected skin.
The first step in the decision
Even though one reaches the point of considering depigmentation, making the actual decision to go forward is not an easy one. Depigmentation is permanent, irreversible. There are many concerns and even fears that naturally arise. For example, will the pigment come back? Are there skin reactions? Do people regret having started the treatment? Are there side effects?
People of non-white ethnicity face additional concerns about loss of racial identity, as well as cultural and social concerns that also must be addressed prior to starting treatment. How will family and friends respond? Will people still accept me if I am a different color?

Before and after photo of a fully depigmented man of Indian descent
There are many testimonials that address these questions and more on the depigmentation forum on our web site. The forum is an excellent resource for those considering whether to depigment, and also contains an overview that is helpful and informative. In this article we review the positive findings of the one published medical study of patient experience with MBEH (the drug used for depigmentation).
What is involved in depigmenting the skin?
Depigmentation therapy is designed to remove the remaining pigment in the skin to match the areas that are already white. For people who have vitiligo on more than 50% of their bodies, depigmentation may be the best treatment option.
A dermatologist must decide whether this treatment is appropriate. A recent survey showed that dermatologists vary in their opinion as to who should be eligible for this therapy. The survey showed that 42% of dermatologists are in favor of depigmentation when vitiligo affects more than 50% of the body, while 32% feel that patients must wait until it affects more than 75% of the body.
In general, depigmentation is limited to the patient for whom repigmentation therapies have failed and/or has more than 50% pigment loss in their skin or when the depigmentation is extensive in the cosmetically sensitive areas of the hands and face. Depigmentation is not generally recommended for children.
 |
The main method used to depigment vitiligo-affected skin is the topical application of monobenzyl ether of hydroquinone (MBEH) (also referred to as monobenzone). MBEH is a topical prescription product applied to the pigmented areas. This is the only drug approved by the FDA for depigmentation therapy of advanced vitiligo. For many years, MBEH was available under the brand name Benoquin, but it has now been discontinued by the manufacturer. MBEH is now only available as a compounded product (monobenzone powder added to a base cream) made by specialized pharmacies. While there are periodic shortages of the monobenzone powder, VSI maintains a list of pharmacies where the compounded cream is generally available.
How is it used?
A cream with a 20% concentration of MBEH is applied twice a day for 3-12 months. It is important to understand that this is a systemic treatment, meaning that regardless of where the cream is applied, it will affect the entire system or body and areas away from the treated area will still lighten. This is not a treatment used to selectively lighten or depigment a specific or confined area. Treatment will generally begin with a concentration of 20% MBEH. Depigmentation should begin after 3 to 4 months of application. The concentration is frequently increased to 30% or 40% during the process, but MBEH concentration greater than 40% is not recommended. If the vitiligo has been stable for years, a longer duration of therapy and higher concentration of MBEH may be required. Direct skin-to-skin contact with other people must be avoided for at least two hours after applying the drug, as transfer of the drug may cause depigmentation of the other person’s skin.
How well does it work?
Until a day or two prior to the date of this VSI Newsletter, the study discussed here was the only one published reporting on the effectiveness of MBEH in the depigmentation of vitiligo patients. It is a retrospective study where researchers at Massachusetts General Hospital in Boston looked back at the experience of 18 vitiligo patients who underwent MBEH therapy. The patients ranged in age from 26 to 68 years of age and had had vitiligo from 6 months to 51 years. Fifteen were women and three were men. Two of the patients were African American and sixteen were Caucasians. The patients had 40 to 90% depigmentation prior to beginning treatment with MBEH. In only one patient was the vitiligo rapidly progressive at the time. The remainder of the patients had stable or slowly progressing vitiligo. The treatment protocol involved the twice-daily application of 20% MBEH.
Of the 18 patients:
Eight (44%) severely-affected vitiligo patients achieved complete depigmentation. Their first signs of depigmentation occurred within one to six months (average under three months) of the start of therapy and full depigmentation was achieved in 4 - 12 months. Furthermore, after six months of MBEH use, one of these eight patients, who had experienced partial depigmentation, continued on to completely depigment after discontinuing MBEH.
Three (17%) had dramatic, though incomplete depigmentation.
Three (17%) experienced partial depigmentation.
Three (17%) elected not to complete the trial.
One (5%) could not use MBEH because of contact dermatitis.
The researchers observed that the average patient in the trial did not begin to depigment until after two-three months or more of application of the MBEH, and also found that the time of the first appearance of depigmentation was not predictive of the final degree of depigmentation. They concluded that consistent use of MBEH correlated with the eventual success of depigmentation. They reported that all those who depigmented fully said they were very pleased with their results. Two of these patients were African American.
In terms of side effects, seven of the 18 patients reported no complications. In two cases, the sensation of burning lasted only the first month of therapy. In two other patients it did limit therapy; however, mixing the MBEH with an emollient helped relieve the burning in these patients. Severe contact dermatitis did cause one patient as described above to drop out of the trial. Other side effects observed were redness or rash, dryness, and swelling.
The study's authors concluded that MBEH was effective, produced generally satisfactory results, and involved limited side effects. They concluded that treatment should lead to an onset of depigmentation within three-six months of therapy being started and full depigmentation within a year. They cautioned that occasional use thereafter may be required.
They also pointed out that during and upon completion of the depigmentation therapy patients are unusually sensitive to sunlight and permanently at risk for acquiring sunburn. Midday sun exposure should be minimized and a sunscreen used to avoid recurrence of pigment that can occur on sun-exposed sites.
Depigmentation and Melanoma
One of the concerns frequently expressed by those interested in depigmentation is whether the process increases their risk of serious skin cancers like melanoma. A study coming out in April 2011 concludes that using MBEH may actually be helpful to prevent the occurrence of melanoma in those with a family history of the disease. Since melanoma is cancer of the melanocytes, and the melanocytes are destroyed by using MBEH, it has long been reported that the risk of melanoma is low to non-existent in those who have completely depigmented. (Source: Dr. James J. Nordlund, Professor of Dermatology, Group Health Associates, Cincinnati, OH and Wright State School of Medicine) Click here for additional information on Vitiligo and Skin Cancer
|
Please see "Medical News and Updates" in this newsletter edition for additional information on the newly released MBEH/Melanoma study. |
An alternate approach
A second depigmenting approach has been reported in the literature, though it is not widely used or available. This approach involves the use of 4-methoxyphenol or mequinol (a phenol derivative), a prescription topical. It is also known as p-hydroxyanisole or monomethylether of hydroquinone (4MP).
How is it used?
The effectiveness of 4MP has been significantly correlated with the duration of the use of the cream. The longer it is used, the better the results. In the only other clinical trial of a depigmentation treatment for vitiligo, topical 4MP produced total depigmentation in 11 of 16 patients (69%) with onset of depigmentation within 4-12 months. Of the 11, four had a recurrence of pigment 2-36 months after concluding treatment. Side effects were mild burning or itching. Four of the five non-responders to 4MP did depigment when treated using a Q-switched ruby laser.
How well does it work?
The onset of depigmentation can occur within 4-12 months, which may be longer than MBEH. Side effects include mild burning or itching, irregular leucoderma and skin irritation. Pigment may return and protection from sunlight is necessary.
Summary
Depigmentation can be effectively achieved. Many who have depigmented their skin have expressed satisfaction. This is not for everyone who has severe vitiligo, but it can be a satisfactory route for those who feel they have exhausted all other options and understand that this process is permanent, irreversible, and that repigmentation therapy is not an option in the future. Anyone considering depigmentation should visit the VSI depigmentation forum to read the experiences of others who have depigmented or are in the process of doing so. If you would like to participate in the forums, joining VSI as a Supporting Member will enable you to post or reply to messages in the many VSI forums. It will also provide access to member photo galleries showing treatment progress; several members pursuing depigmentation have posted in the photo galleries. Click here for more information on the Supporting- level membership. The experiences of our members may vary from the study covered here; their results are generally more positive. It is also important to find a physician who is knowledgeable about vitiligo and who is someone you trust to go through this process with you.
|
To read the personal stories of those who have depigmented or who are
currently depigmenting, log on to the VSI website and visit |
Surgery: An Option For Stubborn Pigment
Although medical therapy has improved considerably in the last years, some people fail to sufficiently re-pigment through medical treatment. Surgical options offer the possibility of repigmentation to a select number of people within this group of non-responding patients. Surgical therapy can provide higher re-pigmentation rates for difficult-to-treat localized areas in selected patients, and can be used to treat generalized disease as well. Repigmentation generally takes several months following the surgery and often more than one surgical intervention is required.
Who would use surgery?

Segmental Vitiligo |
Those people considered the best candidates for surgery are those with stable, segmental or localized vitiligo. They are the most likely to experience a high rate of repigmentation with surgery. Segmental vitiligo affects young people mainly before the age of 20 and is characterized by initial rapid spreading within a confined area, frequently on one side of the body, and then remaining stable.
People with stable, non-segmental vitiligo (NSV) can also respond adequately. NSV frequently results in symmetrical areas and can be generalized over large portions of the body or localized to a particular area. A small percentage of those with NSV may have long periods where the vitiligo remains stable, making them candidates for surgery; for these patients, there is still less than a 50% repigmentation success rate.
Stable disease is an important factor in patient selection for surgery. Stability is generally defined as having no new lesions, no Koebner phenomenon (spreading as a result of skin trauma) and no spreading of the lesions in the previous 12 months.
How is it used?
Repigmentation surgery has the goal of transplanting functional melanocytes (or pigment cells) to the de-pigmented area. This transplantation can be done through one of several methods, each of which harvests the melanocytes in a different way.
Two types of surgical grafts are available
- Tissue Grafts
- Cellular Grafts
Tissue grafts
With tissue grafts, only a limited surface area can be treated, but with good results in the majority of cases. Grafting is suitable for stable patches and can be done in multiple ways using mini-punch grafts, thin-split thickness grafts, and suction blister grafting. Repigmentation can take up to 6-9 months. There are several possible complications that can occur. Infections may occur at the donor or recipient sites. The sites may also develop scarring, a cobblestone appearance, spotty or uneven pigmentation or may fail to repigment at all.
In the tissue skin graft the doctor removes sections of the normal, pigmented skin (donor site) and places them on the depigmented areas (recipient sites). Treating with grafting takes time and is costly, but it does work for some people.
- Mini-punch grafting

|
Owing to its simplicity, minigrafting is one of the most common methods used for vitiligo surgery. After local anesthesia, multiple skin perforations with a small punch are taken from a pigmented donor area; these minigrafts are then harvested and kept under sterile conditions until grafting. The depigmented area is prepared before harvesting the minigrafts by perforating the recipient area with holes from a punch of similar size. Harvested minigrafts are then transferred to the recipient site and the grafted surface is covered with tape to ensure adequate immobilization; the tape is removed two weeks later. Repigmentation occurs gradually after grafting within one month and full repigmentation can be achieved in 3-6 months. An advantage of this method is that because of its simplicity it can be performed by any dermatologist. A side effect of particular concern with this method is cobblestoning, which occurs when the punches used are too large.
- Thin-split thickness guide
This technique has a reported high success rate. With a suitable dermatome (area of skin that is mainly supplied by a single spinal nerve), thin skin grafts may be harvested from the donor site that are then used to replace the depigmented skin. The recipient site is prepared by removing the top layers of skin with superficial dermabrasion (scraping, either by hand or with a laser) and the thin skin sheets are grafted directly onto the abraded area. Grafts are placed next to each other, covered with petrolatum gauze, and secured with surgical wrappings that are kept for one week. Repigmentation is shortly achieved in the following weeks. Difficult areas, such as the hands and fingers, have been grafted with success. An advantage of this method is that it is very simple to perform; a disadvantage is that more than one split skin grafting session can be necessary. Scarring is a possible side effect if the skin sheets used for grafting are too thick.
- Suction blister grafting
In this procedure, the doctor creates blisters on the pigmented skin by using heat, suction, or freezing cold; suction is the most commonly used. The tops of the blisters are then cut out and transplanted to a depigmented skin area. The risks of blister grafting include scarring and lack of repigmentation. However, there is reported to be less risk of scarring with this procedure than with other types of grafting. This form of grafting has reportedly become very popular and is said to yield excellent results. Several publications have reported an absence of side effects and that the donor site can be reused for treating additional areas. Repigmentation occurs gradually; with PUVA therapy, reportedly, repigmentation is enhanced. A review of blister grafts showed that results were significantly better in segmental vitiligo than in the generalized type and in individuals less than 20 years of age. The location of the vitiligo patch did not influence the treatment outcome significantly.
The general published consensus seems to be that, of the tissue grafts, thin-split thickness grafting and suction blister grafting are the best surgical options, as they give the best cosmetic and repigmentation results and utilize surgical facilities that are relatively available. Split-skin grafts have a reported success rate of 78-91%. Suction blister grafting has a reported success rate of 73-88%. Mini-punch grafting, owing to its simplicity, is one of the most common methods used in vitiligo surgery to treat small-or medium-sized lesions. Any dermatologist can perform it, but published expert consensus seems to be that this is the least effective method due to a high incidence of side effects and poor cosmetic results.
Cellular grafts
There are two methods of Cellular grafting:
- Cultured
- Non-cultured
Cultured cellular grafts involve the doctor taking a sample of normal pigmented skin and placing it in a laboratory dish containing a special cell-culture solution to grow melanocytes. When the melanocytes in the culture solution have multiplied, the doctor transplants them to the depigmented skin patches. These in vitro (in the lab) culture techniques can be used to treat extensive areas of depigmented skin as well as localized areas. Extremities of peripheral body areas, such as the dorsal (tops of the) fingers, ankles, forehead, and hairline, and bony prominences do not respond well. While effective, these techniques can be costly and require sophisticated laboratory and surgical support systems. As a result, they are not readily available surgical options in the United States. However, both cultured and non-cultured cellular grafting are more available in other countries such as India and areas of Europe.
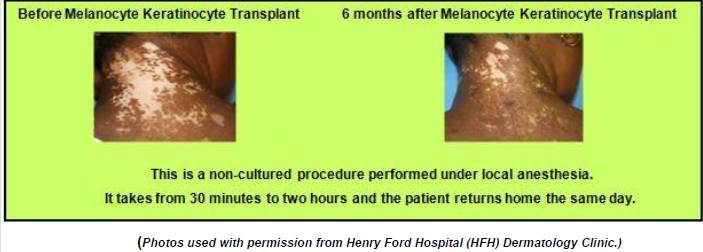
Non-cultured grafts are performed all in one surgery and always include both melanocytes and keratinocytes. The Henry Ford Hospital (HFH) in Detroit just completed a study on non-cultured melanocyte-keratinocyte transplantation and now performs the procedure.HFH reports that this method can cover an area 10 times the size of the donor sample taken. This method also requires less equipment and is an easier process, making it likely that it will be more readily available at some point
The two cellular transplantation techniques are:
Transplantation of melanocytes and keratinocytes
Transplantation of melanocytes only
Transplantation of melanocytes and keratinocytes
(Non-cultured or cultured procedure)
The initial step in this procedure is harvesting a small donor skin sample to provide cells for an epidermal or melanocytes/ keratinocytes suspension. For a non-cultured transplant, the suspension is then placed over the abraded area on the recipient site.
The advantage of the non-cultured method is its relative simplicity, but cost can still be a factor. Numerous small studies have been published reporting good results in the majority of cases with this type of graft. Reported side effects with these options include spotty pigmentation or failure to repigment. Scarring, infection or poor wound healing have also been reported.
Transplantation of melanocytes and keratinocytes can also be a cultured transplant where the cell suspension is seeded in culture flasks with appropriate culture media. Thin epidermal sheets are obtained three weeks later, which are removed from the culture vessel and transferred to the recipient site previously denuded by one of various procedures. After the suspension is spread onto the recipient surface it is then covered for five to seven days until a good cellular take occurs. Reported side effects are similar to the non-cultured transplants.
Transplantation of Melanocytes
Only (Cultured Procedure)
Transplantation of melanocytes only is always a cultured transplant where the cell suspension is seeded in culture flasks with appropriate culture media. Thin epidermal sheets are obtained three weeks later, which are removed from the culture vessel and transferred to the recipient site previously denuded by one of various procedures. After the suspension is spread onto the recipient surface it is then covered for five to seven days until a good cellular take occurs.
Repigmentation is achieved in both types of grafts during the following months, and sunlight exposure or PUVA enhances repigmentation. One of the advantages of the cultured methods is the large population of cells obtained from a small donor site, making them useful to treat extensive areas in a single session, but two disadvantages are the cost and required surgical support systems.
Reported side effects include spotty pigmentation or failure to repigment as well as scarring, infection or poor wound healing. There is some concern with cultured transplants that the growth mediums and culturing process might lead to changes in the cell biology that could make melanoma more likely. So far, lab testing has shown the process to be safe, but further testing must be done.
Summary
Generally, the consensus seems to be that surgery works best on limited, visible areas, including the lips and eyelids. However, some experts feel that surgery is under-utilized as an option, probably because many dermatologists are not experienced in these surgical procedures or aware of their potential usefulness.
Your dermatologist may be able to help you learn if you are a good candidate for this option. If you are considering one of these surgical options and need help finding a doctor who performs a specific procedure, contact VSI.
(VSI would like to thank Marsha Henderson MD, Research Fellow, Department of Dermatology, Henry Ford Medical Center for her contributions and medical review of this article)
Sunscreens:
Pros, Cons & Alternatives
Overview

|
Sun exposure is necessary for all of us. The sun's rays are important to human health. Our vitamin D production, for example, is promoted by exposure to ultraviolet light. Sunlight is also helpful in treating vitiligo-affected skin. Limited, but regular, exposure to the sun is effective for many in repigmenting their skin.
At the same time, limiting the amount of sun one gets is important as well, since too much sun can cause problems. The non-vitiligo-affected skin can be especially vulnerable to the sun's side effects. Sun protection is important and can help limit the skin damage, wrinkles, and the risk of developing skin cancer that comes with long-term, intense exposure to the sun.
Managing the benefits of the sun while still limiting its toxic effects can be a tricky balancing act. There are several ways to protect against overexposure to the sun, such as wearing protective clothing and limiting time outdoors. Wearing sunscreen is another popular sun protection method. However, some scientists and public interest groups have raised questions about their effectiveness and safety. What are the issues and what do we know? Let's begin with effectiveness.
Are sunscreens effective?
Sunscreen use is widely advocated as a means of preventing skin cancer, though human empirical evidence on its effectiveness in this regard is limited. The increasing incidence of skin cancer in many white-skinned populations, despite dermatologist recommendations for several years to always use sunscreen, raises the question for many about how effective sunscreens really are in protecting against skin cancer. For that reason, researchers in England initiated a study to better ascertain how effective sunscreens were in protecting against the effects of the sun.
These researchers found that not all sunscreens were equally effective in protecting against the sun's radiation. Their research showed that broad-spectrum sunscreens offered the best protection against the effects of the sun, especially in temperate latitudes that lie between the tropics and the polar circles. Broad-spectrum sunscreens protect against the effects of both UVB and UVA, as opposed to the majority of sunscreens that just protect against UVB.
|
Why is UVA protection important?
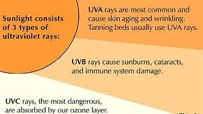
The sun emits ultraviolet radiation in the UVA, UVB and UVC bands. Ultraviolet light A (UVA) and ultraviolet light B (UVB) cause most of the effects, including suntan, sunburn and sun damage. The ratio of UVB to UVA varies with the height of the sun, meaning the amount of UVB exposure versus UVA exposure will vary with latitude, season and time of day. The greatest UVB exposure occurs at the equator (a low latitude), for example. On the other hand, a higher ratio of UVA is commonly found in the higher latitudes as one moves north or south away from the equator into the temperate latitudes and polar regions.
Sunscreens work by absorbing, reflecting, or scattering these ultraviolet radiation emissions, primarily UVB. They are available in many forms, including ointments, creams, gels, lotions, sprays, and wax sticks. All are labeled with SPF (Sun Protection Factor) numbers. In theory, the higher the SPF, the greater the protection from the sunburn caused mostly by UVB rays.
|
|
However, protection against UVA rays, the researchers state, is equally important. Though generally a given dose of UVB is about 1000 times more erythemogenic (producing inflammation and redness of the skin) than the same dose of UVA - which is why most sunscreens are geared towards UVB - one can suffer toxic effects from over-exposure to UVA radiation as well.
|
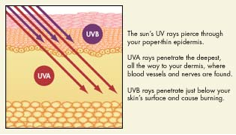
The SPF, however, does not tell us the whole story. It does not tell us which spectrums we are protected against. UVA is a more deeply penetrating radiation than UVB and is believed to also contribute to skin cancer and be capable of causing sunburn, wrinkles and age spots. As it makes up the vast majority of the sun's radiation, scientists have begun to take a closer look at how effectively sunscreens protect against the damaging effects of UVA.
British researchers tested two sunscreens labeled SPF 6 for their photoprotective (sun-protective) abilities on eight young, healthy, fair-skinned adults; one absorbed only UVB and the other absorbed both UVB and UVA (broad-spectrum). They simulated sunlight typical of temperate latitudes (i.e., North America, Northern Europe) where there is a greater ratio of UVA versus UVB. The SPF of each sunscreen was tested against a variety of ranges of solar UVA/UVB that simulated the natural differences found with changes in time of day and latitude. In all instances, the broad-spectrum sunscreen gave much better protection against cumulative erythema (skin redness) than the UVB sunscreen.
If erythema is considered a biomarker of solar skin damage that may lead to skin cancer, then these results suggest that broad-spectrum sunscreens could be advantageous in preventing UV-induced cancer. UVB sunscreens have shown benefit for reducing squamous cell cancer and its precursor, actinic keratosis; however, the data are less clear for melanoma. Whether a broad-spectrum sunscreen would be better in this respect is of substantial interest, but unknown as yet.

|
Why don't most sunscreens specify their protection against UVA?
SPF measurements are based on how well a product would work at high elevations or at low latitudes (equatorial regions) to protect against UVB, which exists at a higher ratio versus UVA in these places. No scale currently exists for UVA protection. The Food and Drug Administration (FDA) is proposing a sun protection factor rating system of one to four stars that may eventually appear on broad-spectrum sunscreen products.
What broad-spectrum sunscreen will give me the best protection?
Consumer Reports tested 12 broad-spectrum sunscreens in 2010 and identified the top four that provided very good UVA protection and excellent UVB protection, and met their SPF claim even after treated skin was in water for 80 minutes. These four are:
| Up & Up Sport Continuous (Target) Spray | SPF 30 $0.88 an ounce | Overall score 88 |
| Walgreen's Sport Continuous Spray | SPF 50 $1.33 an ounce | Overall score 88 |
| Banana Boat Sport Performance Continuous Spray | SPF 30 $1.60 an ounce | Overall score 88 |
| Aveeno Continuous Protection Spray | SPF 50 $2.00 an ounce | Overall score 88 |
Most, if not all, broad-spectrum sunscreens contain some or all of the following ingredients that guard against UVA radiation: avobenzone, zinc oxide, and titanium dioxide. The effectiveness of these ingredients, however, can depend on the formulation.
What are the safety concerns around the use of sunscreens?
While sunscreens are generally believed by medical experts to effectively protect against skin cancer and skin aging, they may also have adverse effects, including contact sensitivity, risk of vitamin D deficiency, risk of over-exposure to vitamin A and hormone disruption, which some public interest groups believe could increase the risk of cancer in those using sunscreens. There is also concern about the use of 'nanoparticles' in the manufacture of sunscreens that, for some, raises the potential for an additional threat to human health.
The FDA, which has the responsibility for approving the use of specific ingredients in sunscreens, has not yet found any of these risks to be sufficiently proven to disapprove or limit the use of sunscreens. However, we recognize there are public concerns, whether theoretical or real, and they warrant a review.
Contact Sensitivity
Although infrequent and subjective, stinging and burning are the most common complaints associated with sunscreens. True allergic contact dermatitis is considered to be rarely caused by sunscreens. Inorganic agents are reported to be unable to penetrate the top layers of the skin, so a dermatitis reaction does not typically occur.
However, there are mixed reports on whether the newly formulated microfine inorganic agents (or nanoparticles) can penetrate the skin layers and if so, what their consequent systemic effects might be.
What are nanoparticles and how do I know if they are in my sunscreen?
Nanotechnology is a growing field and nanoparticles are becoming increasingly prevalent in consumer products, allowing fabrication of stain-resistant carpets, anti-fogging windows, anti-aging cosmetics and transparent sunscreens. Titanium dioxide and zinc oxide, for example, are common mineral-based active ingredients in sunscreens that are often made nano-size because it makes them easier to apply and clear, rather than white/opaque.
As these nanoparticles often exhibit very different properties from their normal-sized versions, there is concern about their possible toxic effects. This concern stems from the debate as to whether nanoparticles can penetrate the skin and be absorbed internally after topical application. Also, no one knows whether ultraviolet light radiation impacts the penetration of these particles into the skin.
Lab studies indicate the potential for these small particles to cause DNA damage and other harm as well. However, research has yet to definitively show that these particles are posing risk to human health when used in sunscreens. Studies suggest they don’t reach live tissue under normal circumstances. One recent study, however, reported preliminary findings that UV-damaged skin may be more susceptible to nanoparticle penetration.
Manufacturers are not required to list nanoparticles, so while sunscreens may contain nanoparticles of zinc oxide or titanium dioxide, you probably won't see the term 'nano' on the labels. Consumer Reports tested 8 sunscreens that contained 'nano' versions of these compounds. Only one, Keys Solar RX, disclosed that they were in nanotechnology form.
How do I avoid nanoparticles in sunscreens?
|
|
If you want to avoid these nano-scale ingredients, there are options. Sunscreens with nanoparticles of titanium or zinc will often have buzzwords such as "clear" on the label, since regular-sized particles make the product white or opaque; titanium dioxide and zinc oxide act as physical barriers against the UV rays. You can also choose from among those called 'chemical' sunscreens that use other active ingredients instead. In its 2007 tests on sunscreens, Consumer Reports pointed out that one of the top-scoring US products, Neutrogena Ultra Sheer Dry-Touch SPF 45, did not contain either zinc oxide or titanium dioxide.
What are the potential risks of chemical sunscreens?
- Hormone disruption and other chemical reactions
|
Several sunscreen agents have been found to affect estrogen and other hormone levels in lab studies. Other studies also suggest that these hormone effects may be amplified in combined sunscreen formulations. No medical consensus exists regarding what this means for people using sunscreens or what the clinical relevance is. Researchers have recommended long-term studies be done to better assess any risk from these hormone effects. Oxybenzone is the agent considered by critics as the most dangerous in its hormone effects.
Critics of sunscreens fear that exposure to sunlight induces further chemical changes in the sunscreen agents that increase the threat of cancer and skin aging. Some fear that a group of chemicals called benzophenones, approved by the FDA for sunscreens, when exposed to ultraviolet light will produce free radicals, which in turn will damage cells, which increase the risk for cancer and skin aging. For those with vitiligo, the production of free radicals could lead to an increase in vitiligo lesions, since many scientists believe that oxidative stress (free radical production) is a factor in vitiligo.
- Vitamin D insufficiency

|
Vitamin D is essential for human health. Vitamin D synthesis requires exposure to UVB. At least 90% of our vitamin D requirement is believed to be derived in this manner. Some suggest that regular sunscreen application may cause vitamin D insufficiency. However, some past studies have shown that long-term sunscreen use has little to no effect on vitamin D levels and function, perhaps because of the incorrect application of sunscreen.
* See study in "Medical News and Updates" (below) addressing impact of proper sunscreen application.
The American Academy of Dermatology (AAD), though, recently revised its position on this, stating that regular sunscreen use may increase the likelihood of developing vitamin D insufficiency and that people using sunscreen could require extra vitamin D through their diet or supplements.
- Vitamin A exposure
Many sunscreens contain vitamin A, listed as retinyl palmitate or retinol on the label. Some public interest groups feel that this increases the public's risk of developing skin tumors and lesions. They base this on a 2009 FDA study testing vitamin A on mice.
Are there other options?
Since sunscreens help protect our skin, we are in the position of having to balance what we need to do to protect our skin from the sun and to minimize or avoid other possible risks posed by some sunscreens' chemical ingredients. Until we know more about the risks sunscreens pose, we will need to continually balance our choices as to what is best for our health. One way to achieve that balance is to not solely rely on sunscreens to protect your skin. There are other things you can do such as:
- Avoid over-exposure to the sun, especially between 10 a.m. and 4 p.m. Seeking shade may help, but it is estimated that 50% of UVA exposure occurs in the shade.
- Do not burn
- Use sun-protective clothing, a broad-brimmed hat and UV-blocking sunglasses.

|
When using a sunscreen, here are some tips to keep in mind:
- Use a broad-spectrum (UVB/UVA) sunscreen.
- Use SPF 30, according to the latest sunscreen review published in the Journal of American Academy of Dermatology.
- Do not lengthen your time out in the sun because you think you are protected by the sunscreen. Sunscreens are not tanning aids.
- Sunscreens should be applied 15 to 30 minutes before exposure. To remain effective, they must be reapplied often, especially when perspiring or swimming.
|
If you want to read more about the safety issues around sunscreens and find what others recommend, visit the Environmental Working Group (EWG) site for a listing of sunscreens that it feels are the safest, as well as information on the concerns raised by critics on the safety of sunscreens.
EWG Sunscreen Guide
VSI will keep you informed of any new findings on the benefits and risks of sunscreens.
Camp Discovery

|
Summer Camp for Kids with Chronic Skin Disease
The American Academy of Dermatology (AAD) is proud to offer six camping sessions for young people with chronic skin conditions who are between the ages of 8 and 16. Under the expert care of dermatologists and nurses, Camp Discovery gives campers the opportunity to spend a week with other young people with skin conditions, while participating in everything from swimming and fishing to horseback riding to lots of camp games and just plain fun! There is no fee to attend this very special camp. Full scholarships, including transportation, are provided by the AAD through generous donations from its members, outside organizations and individuals. All campers must be referred by their dermatologist. Deadline for registration is April 8, 2011, but they have indicated that they will continue to accept applications until each session is full, and they usually have openings after the deadline.
2011 Dates:
- June 26 to July 1, Camp Little Pine in Crosslake, Minnesota (ages 10 to 14)
- June 26 to July 1, Camp Reflection in Carnation, Washington (ages 9 to 16)
- July 10 to 15, Camp Big Trout in Crosslake, Minnesota (ages 14 to 16)
- August 14 to 19, Camp Liberty in Hebron, Connecticut (ages 10 to 16)
- August 6 to 12, Camp Dermadillo, Burton, Texas (ages 9 to 15)
- August 13 to 19, Camp Horizon, Millville, Pennsylvania (ages 8 to 13)
Learn More About Camp Discovery: Click Here
For information about registration, contact Janine Mueller at 847/240-1737 or [email protected]
Click here to read a review of Camp Discovery 2010 from one of VSI's members
Medical News Updates
Highlights of recently-published medical
articles on vitiligo and its treatments
High SPF creams (30+) help compensate for under-application.
Well documented research has shown that most people only apply about 25% of the amount of sunscreen recommended on the SPF product label. Consequently they do not get the degree of photo-protection listed on the label.
Researchers tested the SPF values of four lotions of SPF 30, 50, 70, and 100, and two sprays of SPF 50 and 100. They tested them with four different application amounts, side-by-side on the same panel of subjects to compare the relative efficacies of the different SPF levels.
The results showed that SPF levels are directly correlated with the amount of product applied for all the high SPF formulations, and that high SPF lotions or sprays provide statistically superior protection than lower SPF sunscreens in real life situation when patients under-apply the products.
(February 2011 Journal of the American Academy of Dermatology, Poster abstracts, “The relevance of high SPF products: High SPF sunscreens help compensate under-application.” Curtis Cole, Ph.D., Johnson and Johnson, U.S. For full list of researchers, see Newsletter Bibliography.)
Researchers report that monobenzyl ether of hydroquinone (MBEH), a topical cream used in the depigmentation treatment of extensive vitiligo, has the ability to prevent melanomas.
Because common depigmenting agents are known to kill melanocytes (cells critical to melanoma formation), researchers chose to test both 4-tertiary butyl phenol (4-TBP) and MBEH, both depigmenting agents, as possible melanoma prevention agents.
The ability of both agents to depigment was first tested on mice. MBEH was reported as being the only one that produced significant depigmentation, suggesting a very selective immune response in the skin.
When melanoma cells were injected into MBEH-treated mice, significant retardation of melanoma tumor growth was observed. Effective melanoma prevention requires a depigmenting agent that induces melanocyte death both where the agent has been applied, as well as in distant pigment cells (areas of the body where the cream was not applied).
The researchers concluded the use of MBEH may be suited to prevent tumor recurrences and as a preventive treatment of familial melanoma.
(Hariharan V., et al. (2011) Topical application of bleaching phenols; in-vivo studies and mechanism of action relevant to melanoma treatment. Melanoma Research 21:115-26. See bibliography for full listing of researchers.)
New method of melanocyte transplantation uses hair follicles as a source of the melanocytes rather than a skin sample.
Current methods using non-cultured cell-based transplantation therapies for vitiligo involve taking a donor layer of skin. Since the overall proportion of melanocytes in the skin is low, these techniques involve additional steps. This study looks at follicular unit extraction (FUE) to harvest hair follicles as a source of melanocytes, as it has long been known that repigmentation often comes from the melanocytes in hair follicles. Fourteen patients with vitiligo, stable for at least 3 months, were included in the study. Fifteen to twenty-five hair follicles were extracted from the back of the scalp using the FUE method. The hair follicles were incubated with a trypsin-EDTA solution at 37 degrees Celsius to separate the outer root sheath cells. After filtration and centrifuge to obtain a cell pellet, the pellet was re-suspended and applied to a dermabraded recipient area and covered with a dressing. Overall, 9 out of 14 patients achieved >75% repigmentation. Mean percentage of repigmentation was significantly higher in patients with at least a year of stability than those with less than one year stability. The conclusion was that this method can be a useful simplified transplantation method for vitiligo for patients with stable vitiligo for at least a year, but further evaluation with a larger group is needed.
(Mohanty S, et al (Jan 2011) Non-cultured extracted hair follicle outer root sheath cell suspension for transplantation in vitiligo. Br J Dermatol. doi:10.1111/j.1365-2133.2011.10234.x.)
RESEARCH & CLINICAL TRIALS
Patients Invited to Participate in Online Vitiligo Survey
|
Sponsored by Nanette B. Silverberg, MD Departments of Dermatology, Dr. Silverberg is conducting a survey to review medical, genetic, psychological and nutritional factors that may cause or exacerbate vitiligo. Individuals with vitiligo that have been previously diagnosed by a physician are welcome to contribute to this survey. The survey will not include any personal information that may identify you to the public. Click Link to Select the Appropriate Survey Below Participate in this Survey as an Adult with Vitiligo OR To Participate in this Survey For Your Child |
Major Expansion of Vitiligo Genetics Project
|
UPDATE on International Study to Find Vitiligo Genes |
Scientists with the international VitGene Consortium project spanning 18 countries are working to understand the biology of vitiligo so that more effective vitiligo treatments can be designed. Thanks to your involvement, the first phase of this research project has been very successful, discovering many vitiligo genes, resulting in real breakthroughs in our understanding and opening new doors to developing potential new treatments.
We now plan to expand these studies to discover additional vitiligo genes, giving us even more targets for treatment. That means we need to double the number of patients. Our new goal is to enroll 3000 additional Caucasian (white) vitiligo patients over the next two years. Your help is essential.
If you are from the USA or Canada and have not previously taken part, your participation is vitally needed. Please complete the questionnaire below then email directly to Dr. Richard Spritz at the University of Colorado School Of Medicine using the email address provided at the end of the questionnaire. Your personal information, by law, will be kept private and will not be sold or disclosed. Join with us to work for a vitiligo-free future!
Click here to download the questionnaire
Click Here to Read Research Updates on this Study
|
The Vitiligo & Pigmentation Institute of Southern California Are each conducting a clinical study for a new treatment in vitiligo: an experimental drug to be used in combination with narrowband ultraviolet B (NB-UVB) phototherapy. |
They are looking for adult patients suffering from non-segmental vitiligo on the face and the body, for less than 5 years, and who have never received any kind of light treatment (such as NB-UVB).
The study is composed of a 6-month treatment period with NB-UVB light treatments, performed 3 times a week, with or without administration of the experimental drug.
Thereafter, there will be a 6-month follow-up period with one visit to the testing center every 2 months.
The entire study will last about 1 year and includes NB-UVB light treatment and 11 visits to either the Vitiligo & Pigmentation Institute, or the Henry Ford Hospital Dept of Dermatology
Participation in the study is free and travel expenses will be reimbursed. Your information will be kept confidential.
If you are interested, please contact the center nearest you.
The Vitiligo & Pigmentation Institute of Southern California
Kali Ghazali, CRC
5670 Wilshire Blvd, Suite 650
Los Angeles, CA 90036
(323) 467-4389 ext 6
OR
The Henry Ford Hospital Dept of Dermatology
Marsha Henderson, MD
3031 W. Grand Blvd., Suite 800
Detroit, MI 48202
Research Office (313) 916-6964
[email protected]
Click here for additional information

Whats On Your Mind?
Q. Should I Buy a Used Narrowband UVB (NB-UVB) Light Unit
A. If you are looking to buy a light unit for home use, new or used, there are some things you need to know

|
First, you will need a prescription.
In the United States, where VSI is incorporated and operates, the U.S. Food and Drug Administration (FDA) under Section 201 (h) of the Federal Food, Drug and Cosmetics Act, classifies ultraviolet light units for treating dermatological diseases as "medical devices." As such, the U.S. Code of Federal Regulations Title 21, section 801.109 requires a doctor's prescription to buy (or in any way obtain) a home phototherapeutic device.
Second, it is against the U.S. law for an unlicensed individual to sell a "medical device."

|
U.S. Code of Federal Regulations Title 21, section 801.109 also states that it is illegal to sell, trade, or in any way distribute a phototherapeutic light unit unless legally licensed to do so by the FDA. Under the laws described above, only a physician or licensed light manufacturer or distributor is considered eligible to facilitate a sale or trade of a phototherapeutic light unit.
The point of requiring a prescription is to make sure that the device purchased is fit for the intended purpose (disease) and ensure that the patient is under the direction of a physician when using the device to ensure safe and effective use.

|
Many times VSI receives phone calls or emails from those seeking advice on how to sell their used light unit. As much as we would like to be able to help provide this type of service, we are not licensed by the FDA to be involved in this type of transaction. Another problem we encounter with some frequency is when people post on the forums that they want to sell their light units. As previously explained, in the USA, it is illegal to sell, trade or in any way exchange a phototherapeutic light unit, unless you are registered with, and licensed by, the FDA to do so. Consequently, VSI does not permit these types of posts in our forums. If you have questions regarding the types of posts that are, or are not permitted in our forums, we recommend you read over VSI's Terms of Service, specifically, "Section 6 Website Use and Member to Member Areas (Public Areas)"
To view VSI's Terms of Service: Click Here

|
You also need to be sure that the unit you are buying is legally registered with the FDA. This is important not only to be compliant with the law, but to protect your own health. All phototherapy devices sold in the United States must have a US Food and Drug Administration (FDA) 510K clearance since federal law classifies them as Class II medical devices. The only personal exception that the FDA and U.S. Customs recognize as legal is when one purchases a machine outside the U.S. and hand-carries it back with a valid prescription from a physician.
Manufacturers are required by U.S. law to track the serial number of every device that they manufacture. The recall requirements of the Food and Drug Administration Good Manufacturing Practices (GMP) and European ISO regulations require that they track the serial or batch number of all critical components within the device, such as lamps.
Occasionally, foreign-made knock-off lamps are made that are capable of burning the skin more than a legitimately manufactured and tested narrowband lamp. It can be important to know that the lamps you purchase are not counterfeit or made by companies not complying with the FDA regulations.

|
To counter this tactic and to be compliant with the FDA regulations, Philips, a major producer of ultraviolet lamps, tracks every narrowband lamp they sell in the U.S. and links it to a doctor's prescription. Philips audits everyone that sells lamps or builds machines and checks for prescription records. They are very serious about this 'lifecyle tracking,' as they see that the FDA treats narrow band UVB and broad band UVB and UVA lamps just as they do prescription drugs.
Legitimate U.S. companies spend thousands of dollars a year to remain in compliance with the FDA's standards, which are in place to protect you, the consumer. The companies selling illegal products using illegal methods have not been subjected to these safety measures. The FDA provides a database where you can look up a company to see if it is registered to sell medical devices in the U.S. To check a specific company, Click -- FDA Establishment Registration & Device Listing. This is not a full guarantee, however, that they are being inspected. Each company self-certifies that they are compliant. VSI asks you to boycott illegal companies to protect yourself and American companies who are honoring the law.
|
IN CONCLUSION Selling a home phototherapeutic light unit is illegal if the person trading or selling the unit is not licensed by the FDA to do so, and/or if the purchaser does not have a prescription. |
(VSI would like to thank Daavlin Phototherapy for its contributions to the above information.)
Q. What if I cannot get a prescription that I really need?

|
A. There are different situations that may lead some people to consider acquiring a prescription medication or device either without a prescription, or from a business that does not require a prescription. Just as protections were enacted for medical devices, as described above, the Prescription Drug Marketing Act of 1987 (PDMA) was signed into law by the President on April 12, 1988. The PDMA was enacted (1) to ensure that drug products purchased by consumers are safe and effective, and (2) to avoid the unacceptable risk to American consumers from counterfeit, adulterated, misbranded, sub-potent, or expired drugs.

|
Counterfeit drugs pose potentially serious public health and safety concerns. They may contain only inactive ingredients, incorrect ingredients, improper dosages, or even dangerous sub-potent or super-potent ingredients. Drug counterfeiting is a relatively rare event in this country; however, FDA has seen its counterfeit drug investigations increase to over 20 per year since 2000, after averaging only about 5 per year through the late 1990s.
In the past year we saw nationwide shortages of several ingredients necessary for popular vitiligo treatments. There are also times a person can find it difficult to locate a dermatologist to write a prescription for an approved vitiligo treatment, or those who may have a prescription for a product, but think they can save a few dollars by purchasing from one of these unregulated operations. Purchasing from a business not meeting FDA guidelines most often means the product being sold, whether it is a light unit or medication, does not meet the required safety and testing guidelines.
|
|
By going around the law, the buyer is making a purchase outside of the protections of the law and its safeguard. Aside from the illegality of such a purchase, this also puts their health at risk.
If you find yourself in a situation where you cannot get a doctor's prescription or cannot find a prescription medication or device, contact VSI. We may be able to help you with information on where to find products, especially in those instances when there is a shortage, or help you find a doctor willing to work with you to get appropriate medication for your situation.
|
For additional information on the "Prescription Drug Marketing Act of 1987" - Click Here For additional information on the FDA's "Initiative to Combat Counterfeit Drugs" - Click Here To View the Spring Newsletter Bibliography - Click Here |
Earn Funding for VSI when you shop!
Please keep VSI in mind when you do any of your online shopping
Amazon.com has all kinds of items in addition to books. As long as shopping is done through this link, Amazon.com , or from the Amazon box on our Community Home Page, Amazon returns a portion of the sale to VSI. The more items members buy, the higher the percentage!
Our Vitiligo Library and Store is also powered by Amazon. It contains books, articles and products for those with vitiligo.
Our other program is iGive.com. The iGive shopping mall has over 700 stores where you can shop and VSI gets a percentage. Let friends and family know about iGive, so they can support VSI, too. You do have to register for iGive. Once you've registered, you can either shop directly through their "mall" on iGive's website or by downloading their toolbar, which makes it even easier. iGive also has a search function powered by Yahoo at isearchigive.com that earns VSI a penny per search. The power of numbers makes this also an effective way to support VSI.
![]()
|
You Can Make a Difference Today, for Someone in the Vitiligo Community There is no other source available that offers the comprehensive vitiligo education and patient support as VSI By making a donation to VSI as a Supporting Member; your gift will make a difference in the life of another person living with vitiligo. Over 100,000 people with vitiligo contacted VSI last year for help. We respond daily to hundreds of people coming to us for information and support. As we depend on donations from the public to serve vitiligo patients, your gift is critically needed. When you join as a Supporting Member, you will have the satisfaction of knowing you are helping others whose lives have been affected by vitiligo. You will also gain additional Supporting Member Benefits. If you are already a Supporting Member, an additional gift is welcome and gratefully appreciated. Thank you for your support and for enabling us to provide critically-needed services to this community. |
Reproduction or republication strictly prohibited without prior written permission