For best view, click Fall Newsletter to open in browser.
 |
|||||||||||||||||||||||||||
|
This Newsletter Has Been Generously Sponsored By:

Click Above for More Information on Home Phototherapeutic Light Units for Vitiligo
|
|||||||||||||||||||||||||||
|
Dear Members and Friends of VSI, Have you wondered how your doctor may come to a treatment recommendation for you? What factors influence the decision? There can be several, but the most important is the severity of your vitiligo. In our main newsletter article, we show you how vitiligo experts determine the severity of one's vitiligo. Walking through the steps of the calculation does require a little patience, but, once mastered, gives you a tool that will help you better communicate with your physician. Equally important, knowing how to calculate the severity of your vitiligo can also help you track the effect of your vitiligo treatment over time. We also review secondary factors that can influence what treatment is the best choice for you. Understanding all these factors will put you in the best position to evaluate your options and to communicate effectively with your doctor. We want to hear from you about whether there were factors not included in this article that influenced your treatment decision. Did you know that having melasma may actually be a benefit for those with vitiligo, or that treating your heartburn might lead to pigment loss? If you want to learn more about these issues, or about how Protopic has been shown to work better on some skin types than others, be sure to read the "Medical News Updates" below. Has cost ever kept you from filling a prescription? Would you like to find out if you qualify for free or reduced price prescriptions? Find all this and much more as you read VSI's Fall Edition Newsletter!
Sincerely, Jackie Gardner
 The effectiveness and risk of a vitiligo therapy is directly related to the size of the treatment area(s). For example, a therapy that is very effective in repigmenting small areas of your skin may be much less effective treating large areas, and may also pose more risk. Topical steroids are a great example of this type of therapy. Knowing the amount of pigment loss, and being able to express that in quantifiable terms, is an important first step in determining which therapies are the most appropriate for you as a vitiligo patient. The Vitiligo Area Scoring Index (VASI), a measuring tool used by leading vitiligo researchers and clinicians, gives you a way to make this calculation. Using this tool can help you share a common language with your doctor when defining the severity of the vitiligo and in working with your physician in comparing, and selecting among, the different treatment options. VASI: How it works Calculating the degree of your pigment loss using the VASI may seem daunting at first, but it is an easy tool to use. Even if you decide not to use this tool routinely, understanding the VASI can help you get a general impression of your percentage of skin that is involved and how that correlates with choosing your best treatment option. To calculate the total pigment loss you will need to know two things:
There are four steps used to determine the total 1. Determine the BSA affected. To do this, you need to divide your skin surface into the following six separate regions:
2. Determine how much BSA is involved with vitiligo for each specific region. The affected areas in each region are measured in hand units (a hand unit is defined as the size of the palm and is equal to 1% of the body surface). For example, if the surface area of involved skin is equivalent to five hand units, 5% of the body is considered involved with vitiligo.
3. Determine the percentage of depigmentation for each area. The percentage of depigmentation is calculated to the nearest one of the following percentages: 0, 10, 25, 50, 75, 90 or 100%. (See the percentage definitions below:)
4. Determine the total depigmentation for the whole body. To determine the total depigmentation percentage for the entire body, you
Working example of VASI formula: If the Upper Extremities region has 2 hand units (2%) of BSA affected, and is .75 (75%) depigmented, then the total depigmentation for the Upper Extremities is 1.5% of the body. (.75 x 2 = 1.5%) If the Face/Neck region has 5 hand units (5%) of BSA affected, and the depigmented areas are 1.00 (100%) depigmented, then the total depigmentation for the Face/Neck is 5% of the body. (5 x 1 = 5%) The total depigmentation for the entire body is found by adding the totals together.
Frequently people may describe their depigmentation as covering 90% of their body when what they actually mean is that (in their assessment) 90% of their body has at least some involvement. However, the physician could see it as less severe and recommend different therapies than what the patient might be expecting.
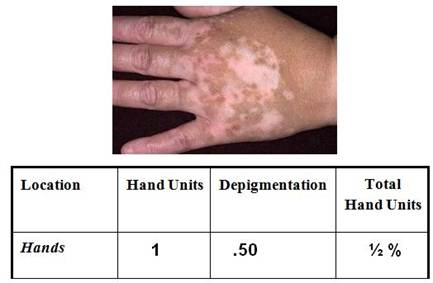
Working examples on calculating pigment loss Hand
Upper Extremities
Working example on calculating pigment loss
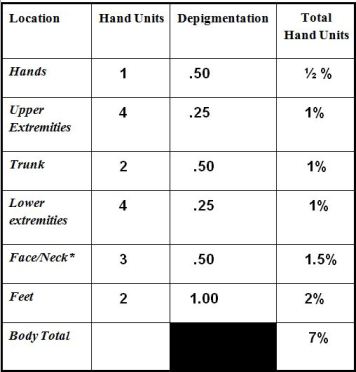
Working examples on calculating pigment loss for the entire body: Liz Liz has vitiligo patches on all 6 regions of her body. Liz feels her vitiligo is covering most of her body, but her doctor says her total pigment loss is only 7%. Why the difference? Though several areas of her body are involved, her BSA involved is limited and only a few sites are completely depigmented.
Reminder: A hand unit is equal to 1% of the body’s surface area. Thus, 7 hand units is equal to saying 7 % of the body surface area (BSA) is depigmented.
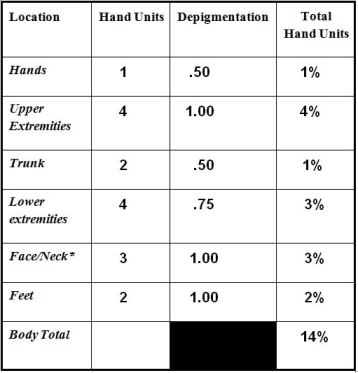
John John’s vitiligo involves the same BSA as Liz, but he has more depigmentation. Thus, the doctor rates John as having a higher percentage of depigmentation. Here is how the doctor calculates John’s vitiligo:
How do doctors use the BSA in selecting treatment? The Body Surface Area (BSA) calculated by the VASI is the first criteria the physician uses in selecting the most appropriate treatment. Treatments will vary depending on how extensive the vitiligo involvement may be. Generally, the rule of thumb for the physician is that depigmentation involving 10% or less of the skin (or BSA) is treated by topical therapy. Combination therapy with topical and light is usually considered when more than 10% of the skin is depigmented. Generalized depigmentation of more than 50% of skin may best be treated by depigmentation therapy. The physician will consider other secondary factors as well in developing a specific treatment plan for each person. These factors can include:
The patient’s age: A patient’s age can affect selection of treatment. For example, though high-strength topical steroids have been reported to be effective in children, use of less potent steroids is often preferred in children under the age of 10 to minimize risk. A systemic steroid would not be used in a child.
Date of disease onset: Some therapies work best when used early in the disease process or soon after disease onset. Topical steroids, for example, are considered to be most effective on small, newly de-pigmented areas, especially those on the face and neck which are areas that respond best to all therapies. As re-pigmentation of patients with long-term vitiligo can be more difficult to achieve, the patient can be advised as to what to expect and the physician can design a treatment approach taking this into consideration.
If the vitiligo is actively spreading, the goal of treatment is to stabilize the disease before trying to repigment. Powerful systemic treatments like full body narrow band-UVB or systemic steroids can potentially provide enough suppressing effect to stabilize active generalized vitiligo and prevent new areas of depigmentation. Topical tacrolimus ointment (Protopic) has also been shown to be most effective when treating active vitiligo.
Type of vitiligo: People with segmental vitiligo may be good candidates for surgical treatment. Those with non-segmental vitiligo would most likely to be treated with topicals and light.
Location of vitiligo: Generally, results of any treatment are better on the face and neck, followed by the trunk, upper arms, and upper legs. Feet and hands are among the most difficult to treat. Topical creams or ointments, and light treatment are often prescribed for the more responsive areas. Surgical options can be considered for the less responsive areas.
The patient’s ability to pay (and their insurance coverage): There are some vitiligo treatments more difficult to have covered by insurance, such as Protopic and the excimer laser. The physician would need to discuss this with the patient before initiating therapy.
The patient’s life style and ability to comply: For example, can a businessman or mother of young children, or even an elementary-aged child go to a doctor’s office three days a week to use their light unit?
Also, how is the patient feeling, what emotional pressures is the vitiligo causing? The emotional stress of vitiligo can have a very direct impact on the quality of life and should also be taken into account. Even a small percentage of involvement can cause a great deal of emotional stress, particularly if more visible areas are affected. Under these circumstances, a doctor may consider a treatment prescribed more often for widespread vitiligo, such as a combination of a topical and light.
Summary The VASI can be a useful way for those with vitiligo to more closely estimate the percentage of their depigmentation and understand which treatments may or may not be the best options.
Do You Need Help Paying For a Prescription Drug?
For people with chronic disease, like vitiligo, who also have limited ability to pay for the brand name drugs they may need, PAPs are a good option. PAPs are generally sponsored by drug companies to help people buy their brand name drugs, in hope that in the future these people will be able to afford them and will want to use their products. You can contact the companies through their web sites regarding their drug assistance programs to see if you meet their requirements for financial assistance. You may also start elsewhere on the Internet. Three web sites in particular serve as major portals to multiple PAPs, and can help you find one that meets your needs: RxAssist, the Partnership for Prescription Assistance, and NeedyMeds. Another good site is RxHope, a web-based patient assistance resource, providing processing, fulfilling and tracking of patients’ requests. Protopic, a prescription brand topical drug that is used to treat vitiligo, is expensive and can be difficult to get covered by some health insurers, as it is approved by the Food and Drug Administration (FDA) only for the treatment of eczema. If your physician has recommended this drug, your health insurer does not pay for it, and you need help in paying for this drug, visit the web site of the drug’s manufacturer, Astellas, to see if you qualify for help under its program.
New Sunscreen Labeling to Help Consumer Sunscreen Labeling According to 2011 Final Rule: The two products pictured here have not been shownto protect against skin cancer Only products labeled with both “Broad Spectrum" AND SPF 15 or higher Starting in the summer of 2012, sunscreen manufacturers will have to meet a uniform and stricter labeling standard that should put consumers in a better position to know which products offer the best protection from the harmful rays of the sun. For the first time, sunscreen products will have to meet certain standards to make health claims and offer specific product facts on their labels. This should make it easier for consumers to compare products and purchase the level of protection they are looking for. Dr. Warwick L. Morison, professor of dermatology at Johns Hopkins University and chairman of the photobiology committee for the Skin Cancer Foundation, tells VSI: “the main benefits these new standards provide for consumers are that we will now have clearly defined broad-spectrum protection from sunscreens against both UVA and UVB radiation and also better labeling regarding water-resistance.” Sunscreens offer different types of sun protection and in varying strengths. Currently, they can all claim to offer protection against skin cancer and skin aging, even though some protect only against sunburn caused by ultraviolet light B (UVB) radiation. The UVB rays cause sunburn and skin cancer; however, UVA rays cause wrinkles and photo-aging as well as skin cancer. For years, consumers have relied on a sun protection factor (SPF) rating, which ranged from 2 to 50 and higher, not realizing that the SPF rating only referred to protection from the UVB rays. If your sunscreen says "SPF 15," then that designation means that it provides fifteen times your natural protection against UVB rays. There has been no rating system for UVA protection, but the FDA has now determined that sufficient data are available to establish a "broad-spectrum" test for determining a sunscreen product's UVA protection. Under the new rules, sunscreens will be required to pass the FDA's broad-spectrum test in order to claim that they protect against both UVA and UVB. Passing the broad-spectrum test will show that the sunscreen product provides UVA protection that is proportional to its UVB protection. The higher SPF levels will provide higher levels of both UVB and UVA protection. Additionally, manufacturers may no longer identify their products as “sunblocks,” as this overstates their effectiveness. Sunscreens also will not be permitted to claim to provide sun protection for more than 2 hours without reapplication or to provide protection immediately after application (for example—“instant protection”) without submitting data to support these claims and obtaining FDA approval. Travel-friendly SPF wipes, towelettes and shampoos, popular with many consumers for their ease of use, can no longer claim SPF protection. Also, manufacturers will not be able to label their sunscreens as “waterproof” or “sweatproof,” as all sunscreens eventually wash off; 'water/sweat-resistant' must be used instead. Other safety issues: Sunscreen ingredients The FDA, in its announcement of these new labeling standards, also addressed consumer concerns about the safety of nanoparticles in sunscreens. Titanium dioxide and zinc oxide, for example, are common mineral-based active ingredients in sunscreens that are often made nano-size because it makes them easier to apply and clear, rather than white/opaque. As these nanoparticles often exhibit very different properties from their normal-sized versions, there has been concern about whether nanoparticles can penetrate the skin and be absorbed internally after topical application. Lab studies have indicated the potential for these small particles to cause DNA damage and other harm as well. Additionally, it said that the safety of the other sunscreen agents, such as chemical sunscreens, that are approved for use in the US would also be re-examined, though it currently had no information suggesting that they are not safe. It is also looking into, and soliciting data on the benefits and risks of sunscreen sprays as to their effectiveness and safety from inhalation risks.
The FDA is considering limiting the top SPF rating to 50+ as there is not sufficient data showing that anything above 50 provides greater protection. In particular, it is asking whether there are special groups of people who would somehow benefit from having a product with an SPF of more than 50. Dr. Morison further commented: “I am disappointed that the FDA has thus far failed to ban SPF numbers higher than 50 because such products expose people to more irritating sunscreen ingredients without meaningful added protection.” The proposal was open for public comment at regulations.gov until September 15th, 2011. After that date, the FDA began review of submitted data to determine their final ruling.
For more detailed information on sunscreen safety and how sunscreens work, see our article on sunscreens in VSI’s Spring 2011 newsletter. In this article, we describe some of the research behind the broad-spectrum issue, and the various consumer and scientific concerns around sunscreens.
Highlights of recently-published medical
Drugs used to treat gastric acid disorders, such as Prilosec and Prevacid, have been linked in various medical reports to causing vitiligo depigmentation and to slowing repigmentation from therapy. They treat ailments such as dyspepsia, peptic ulcers, and gastroesophageal reflux disease (GERD), among others. Also known as proton pump inhibitors (PPIs), they are among the most widely-selling drugs in the world. The latest of these reports describes the re-occurrence of depigmentation in a young female vitiligo patient who took a gastric acid drug after successful repigmentation surgery. The young female patient, 24 years old with generalized vitiligo, had experienced more than 90% repigmentation following a transplantation surgery. She was followed up regularly with no new lesions appearing. However, almost one year after the surgery, she developed hypopigmentation to depigmentation in the repigmented areas after starting oral pantoprazole (a PPI) for gastritis, a drug her general physician had prescribed a few weeks earlier. When she stopped taking the drug, the hypopigmented and depigmented areas repigmented. PPIs are used widely in general practice and may also be prescribed by a dermatologist to prevent gastritis from anti-inflammatory agents used with melanocyte transplantation. Given the wide use of these gastric acid-treating agents, the physician and vitiligo patient need to know about the risk of depigmentation from these drugs. Topical tacrolimus is more effective for
One of the challenges in starting a vitiligo patient on therapy is determining the best initial therapy for any one patient. The findings here, the researchers say, show that topical tacrolimus is a beneficial therapy in all skin types, but may be especially effective for individuals of intermediate skin color (types 3-4). The researchers recommend that more research be done into comparative responses by skin tone and ethnicity to develop ideal therapeutic protocols for vitiligo in individuals of all skin types and ethnicities. Familiar eye drop reported to repigment skin At the World Congress of Dermatology, Indian researchers reported that a topical eye solution, bimatoprost, shows promise as a novel treatment for localized, stable vitiligo. In a small pilot study of 10 patients with localized vitiligo, bimatoprost 0.03% ophthalmic solution was applied, one drop per two cm2 of affected skin, twice daily for four months. Beginning after an average of two months of treatment, seven of the 10 patients showed pronounced repigmentation: three patients had 100% repigmentation, three others had 75%-99% repigmentation, and one patient showed 50%-75% improvement. Patients with disease duration of six months or less had the best results. Lesions on the scalp and face repigmented fastest, after just 4-6 weeks of treatment. Facial lesions responded best, as all three patients who had 100% clearing had vitiligo on the face. During six months of follow-up, three patients with lesions on the trunk or extremities that initially responded to treatment relapsed, typically 2-3 months after conclusion of the 4-month treatment period. Interestingly, all five patients with focal or segmental vitiligo had either 100% repigmentation or 75%-99% improvement, and none relapsed off therapy. The only treatment side effect was a transient burning sensation, mainly on the lips, reported by two patients. Eye researchers reported that these pigmenting side effects were more pronounced with bimatoprost than other topical prostaglandin analogues, which is why the investigators decided to conduct this first-ever study of the drug as a treatment for vitiligo. The long-term effects of daily bimatoprost for vitiligo will require further study. Patients with vitiligo and melasma have a Indian researchers treated patients with vitiligo and those with both vitiligo and melasma with narrow-band (NB) UVB. They found that patients having both vitiligo and melasma had a significantly greater response on the face and limbs, achieving repigmentation much earlier and attaining a greater level of repigmentation than those with vitiligo alone. Although the vitiligo-melasma group started repigmenting earlier on the trunk of the body, unexpectedly the final pigmentation was more extensive in the vitiligo alone group. At the end of 12 weeks of therapy, 86% of patients in the vitiligo/melasma group attained more than 75% pigmentation on the face as compared to only 12.5% of patients in the vitiligo group. Over the limbs, 73% of patients in the vitiligo/melasma group attained more than 75% pigmentation compared with only 9% in the vitiligo group. On the trunk, only 20% of vitiligo/melasma patients showed more than 75% pigmentation compared with 63% of patients in the vitiligo group.
Major Expansion of Vitiligo Genetics Project
What's On Your Mind? Q. How do I know when it’s OK to stop treating an area that has repigmented? A. If you continue to treat an area for several weeks after you are no longer able to tell the difference between the previously depigmented skin and the surrounding unaffected skin, you should be able to stop. If the new pigment has completely filled in the area, but is a bit lighter in color, this is called trichrome vitiligo and is considered to be a stage of active vitiligo. It would be wise to continue treating this area until the color matches the surrounding unaffected skin. Q. I have melasma and vitiligo. What should I do? A. First, let’s define melasma:
There are three types of melasma; epidermal (brown), dermal (blue-gray), or mixed epidermal/dermal (brown-gray).Epidermal melasma is the most outwardly visible and is the most responsive to treatment. Melasma may be confused with the hyperpigmentation some vitiligo patients see around the edges of a depigmented lesion. Most of the topical agents used to treat vitiligo, as well as phototherapy, can cause the hyperpigmentation seen at the edge of the lesion.
Q. What melasma treatments are acceptable for those with vitiligo? A. The difficulty, of course, is that vitiligo treatments stimulate melanocytes and melasma treatments inhibit pigmentation. A vitiligo patient with melasma undergoing light treatments should apply sunscreen on the melasma prior to the treatment. If the melasma is next to or very near the vitiligo, once the vitiligo treatment is finished and the pigment has been stable for several months, one can then consider treating the melasma with alternative treatments such as a light chemical peel or azelaic or kojic acid, all of which must be very carefully administered by a qualified dermatologist.
Q. Can I use hydroquinone to treat the melasma?
Q. Is there a safe treatment (for vitiligo patients) to lighten the hyperpigmentation at the edges of a depigmented lesion? A. When you treat vitiligo, you see two different patterns of repigmentation. One scenario is the activation of pigment cells within the lesion (freckles) to restore color. The other is the stimulation of melanocytes at the edge of the lesion, and they then migrate to repigment the area (a bit slower than the first scenario). On occasion the new pigment may appear darker, or hyperpigmented. This is normal, and in time the color generally evens out. However, if it is particularly bothersome, you can carefully apply sunscreen over the hyperpigmented areas before light treatments. Although this may slow the response, it doesn’t affect the repigmentation of the vitiligo areas. That way you stimulate pigmentation in the lesion without enhancing the hyperpigmentation. (VSI would like to thank Nanette Silverberg, M.D., Attending Physician, Department of Dermatology, St. Luke's-Roosevelt and Beth Israel; Anand Ganesan, M.D., Ph.D. Assistant Professor, Department of Dermatology at the Dermatology Center of UC Irvine; and Ray Boissy, Ph.D., Professor of Dermatology & Cell Biology and Director of Basic Science Research at the University of Cincinnati College of Medicine (UCCOM) for their contributions to this article.)
However from time to time we receive written questions via email in other languages such as Portuguese, Turkish, Romanian, Polish, Greek, Italian, French, German, and Ukrainian. If you are fluent in written English, can translate any of these or other languages, and would be willing to translate written questions and replies on an occasional basis for VSI, please reply to us at [email protected] with the words “Volunteer Translator” in the Subject line.
One of the most often asked questions VSI receives is:
We began surveying other small nonprofit organizations for ideas of alternate ways to implement personal support on a smaller scale that would not exceed our current capacity. If you have vitiligo, you have most likely at some point, experienced the feeling of being alone in a world where no one understands. Vitiligo can seemingly pull the rug completely out from under even the most well-adjusted person, leaving feelings of insecurity and helplessness. We talk with people daily who find it hard to believe they could ever regain the emotional stability they once knew and enjoyed. The road back to a full and happy life is paved with small stepping stones. Sure, there will be bumps in the road, but learning to recognize the bumps and how to move around them will put most people back on track.
Contact information must be complete and verifiable in order for VSI to proceed with the process. If you’re interested in becoming a volunteer, please click below and fill out the online application as completely as possible.
Please keep VSI in mind when you do any of your online shopping
|
||||||||||||||||||||||||||
| Copyright © 2011 Vitiligo Support International Inc. All rights reserved. Reproduction or republication strictly prohibited without prior written permission A Vitiligo Support International, Inc. financial statement is available upon written request from the Virginia Office of Consumer Affairs. Mail requests to: Virginia Department of Agriculture and Consumer Services, Office of Consumer Affairs, P.O. Box 1163, Richmond, Virginia 23218. |
|||||||||||||||||||||||||||



 You may qualify for a Prescription Assistance Program (PAP), offered by most drug companies and some state governments; there are also some PAPS for people with certain diseases or conditions. PAPs are also called Patient Assistance Programs.
You may qualify for a Prescription Assistance Program (PAP), offered by most drug companies and some state governments; there are also some PAPS for people with certain diseases or conditions. PAPs are also called Patient Assistance Programs.

 Gastric acid drug induces vitiligo depigmentation
Gastric acid drug induces vitiligo depigmentation While vitiligo affects all races and ethnicities, there has been limited study of whether skin color affects the efficacy of therapy. In this study, doctors found that skin color did influence the effectiveness of tacrolimus (US brand name Protopic, Tacroz Forte in India), an often prescribed topical vitiligo therapy. They reported that repigmentation was good in all skin types, on the body as well as the head and neck, with greater repigmentation of lesions on the body in people of skin types 3-4 (intermediate skin color).
While vitiligo affects all races and ethnicities, there has been limited study of whether skin color affects the efficacy of therapy. In this study, doctors found that skin color did influence the effectiveness of tacrolimus (US brand name Protopic, Tacroz Forte in India), an often prescribed topical vitiligo therapy. They reported that repigmentation was good in all skin types, on the body as well as the head and neck, with greater repigmentation of lesions on the body in people of skin types 3-4 (intermediate skin color).  Bimatoprost is sold by prescription under the name of Lumigan and is used to control the progression of glaucoma and to manage eye pressure. It is also sold as a prescription treatment under the brand name Latisse to lengthen eyelashes. When used to treat glaucoma, topical prostaglandins such as bimatoprost were found to increase melanin production as evidenced by their common side effects: skin darkening around the eyeball, excess growth of hair, and darkening of the iris.
Bimatoprost is sold by prescription under the name of Lumigan and is used to control the progression of glaucoma and to manage eye pressure. It is also sold as a prescription treatment under the brand name Latisse to lengthen eyelashes. When used to treat glaucoma, topical prostaglandins such as bimatoprost were found to increase melanin production as evidenced by their common side effects: skin darkening around the eyeball, excess growth of hair, and darkening of the iris.
 Melasma is a complex disease most often characterized by a dark skin discoloration appearing on sun-exposed areas of the face, and is especially common in pregnant women, women who are taking birth control pills (oral contraceptives), hormone replacement therapy (HRT) during menopause, or certain anti-epilepsy drugs. Sun exposure is also a contributing factor for melasma.
Melasma is a complex disease most often characterized by a dark skin discoloration appearing on sun-exposed areas of the face, and is especially common in pregnant women, women who are taking birth control pills (oral contraceptives), hormone replacement therapy (HRT) during menopause, or certain anti-epilepsy drugs. Sun exposure is also a contributing factor for melasma. A. Hydroquinone (HQ) (a derivative of Monobenzylether of Hydroquinone (MBEH) used to depigment vitiligo patients) is toxic to melanocytes, thereby causing a gradual decrease of melanin pigment production. Some doctors are adamant that hydroquinone never be used on vitiligo patients, while others will prescribe it in the lower strengths (4%). Because of the sporadic irritating capacity of HQ and some data demonstrating potential carcinogenesis, HQ has been banned in Europe and Asia. It is expected that HQ may soon be banned from use in the US as well, to be replaced by a safer product.
A. Hydroquinone (HQ) (a derivative of Monobenzylether of Hydroquinone (MBEH) used to depigment vitiligo patients) is toxic to melanocytes, thereby causing a gradual decrease of melanin pigment production. Some doctors are adamant that hydroquinone never be used on vitiligo patients, while others will prescribe it in the lower strengths (4%). Because of the sporadic irritating capacity of HQ and some data demonstrating potential carcinogenesis, HQ has been banned in Europe and Asia. It is expected that HQ may soon be banned from use in the US as well, to be replaced by a safer product. VSI receives questions from people all over the world. Though we only speak English, we do have someone who can provide a written translation for questions that come to us in Spanish.
VSI receives questions from people all over the world. Though we only speak English, we do have someone who can provide a written translation for questions that come to us in Spanish. VSI recognizes that the need is great for this type of personal resource, but to date we have not had the funding or manpower to offer physical support groups.
VSI recognizes that the need is great for this type of personal resource, but to date we have not had the funding or manpower to offer physical support groups. Along with a supportive family and medical professional, what better help to get back on your feet than someone who’s been down the same bumpy road and has successfully emerged on the other side? As a result, we’d like to recruit a group of people who would be willing to talk personally, by phone or email, to those who need some emotional support. VSI would screen those requesting assistance to make sure that professional help is not required.
Along with a supportive family and medical professional, what better help to get back on your feet than someone who’s been down the same bumpy road and has successfully emerged on the other side? As a result, we’d like to recruit a group of people who would be willing to talk personally, by phone or email, to those who need some emotional support. VSI would screen those requesting assistance to make sure that professional help is not required.